


Global perspective in reconstructive rhinoplasty - unique challenges from overseas
 0
0 
Abstract
Reconstructive rhinoplasty, beyond its aesthetic role, is vital for the restoration of form and function in low-resource settings. Low- and middle-income countries (LMICs), especially in sub-Saharan Africa, remain critically under-resourced, with fewer than one plastic surgeon per 100,000 population and pronounced rural-urban disparities. Traditional outreach vertical models provide short-term relief but often lack continuity. Diagonal models, with integrated training and outcome monitoring, have demonstrated greater sustainability. Additional consideration is required for rhinoplasty procedures that account for cultural aesthetic norms and regional anatomical variations, as these are associated with higher patient satisfaction and better community uptake, highlighting the importance of culturally appropriate care in global surgical outreach. This narrative review aims to (1) highlight LMIC-specific challenges, particularly in sub-Saharan Africa; (2) compare surgical outreach models; (3) propose sustainable capacity building strategies, and (4) review culturally specific rhinoplasty techniques. As culturally specific rhinoplasty grows on a global scale, the result of locally empowered rhinoplasty surgeons in LMICs through diagonal partnership models and long-term skills transfer will result in improved patient care access. Investment in training, tele-mentorship, and metric-driven follow-up is essential to improving surgical equity and outcomes.
Keywords
INTRODUCTION
Reconstructive rhinoplasty is essential across all socioeconomic contexts. It is not merely a cosmetic intervention but often a functional necessity which restores airway patency, facial symmetry and psychological well-being. Access to surgical care in low- and middle-income countries (LMICs) remains profoundly unequal, with 34.8% of the global population receiving only 3.5% of all surgical procedures[1]. The Lancet Commission on Global Surgery estimated that 5 billion people worldwide do not have access to safe and affordable surgical care[2]. The Lancet reviewed the global distribution of surgeons and found that 48% of the world’s population lives in LMICs, but only 19% of all surgeons practice in these regions[3]. In the 31 World Bank-defined low-income countries (LICs), there are only 63 registered plastic surgeons in total; 16 countries lack any registered plastic surgeon[1]. Notably, 55% of surgical care in LMICs is provided by charitable organizations[1], underscoring the ongoing critical role of outreach and support.
While burn injuries are quoted as the most common pathology treated by plastic surgeons in LMICs (67%), the burden of congenital and traumatic facial deformity is significant, often underreported, and represents a largely unmet care need[1]. Functional septorhinoplasty is a critical skill for the reconstructive surgeon in these settings to address this care gap.
The scope of rhinoplasty beyond aesthetics
Most commonly known for its aesthetic applications, septorhinoplasty surgery involves greater depth and complexity when functional and ethnic considerations are taken into account. Reconstructive nasal surgery dates back centuries, with a description of forehead flap rhinoplasty from 600 BC in India. The first Renaissance-era rhinoplasty dates back to 1887 in Europe when John Orlando Roe described a simple procedure to correct the pug nose via an endonasal approach[4]. Since then, the field has evolved significantly to incorporate functional, aesthetic, and ethnic considerations, particularly relevant in diverse global populations. Over the 20th century, open techniques and graft augmentation have refined outcomes. The evolution of rhinoplasty technique has shifted to preserving ethnic identity while enhancing function[4].
Understanding anatomical variations in the non-Caucasian population is critical[5], as regional and ethnic differences in skin thickness, cartilage structure and healing influence both surgical planning and outcomes. Additionally, regional trauma trends inform surgical priorities[6]. In high-trauma settings, the need for reconstructive nasal surgery is magnified.
This paper explores the unique challenges of reconstructive rhinoplasty in low-resource settings through a review of the literature and collaborative experience, with a focus on sub-Saharan Africa.
SEARCH STRATEGY
This review was designed as a systematic review with narrative synthesis aimed at synthesizing current evidence on surgical outreach models, trauma burden, access to facial plastic surgery (including rhinoplasty), and culturally specific considerations in LMICs.
A structured literature search was performed in PubMed, PubMed Central (PMC), and Excerpta Medica Database (EMBASE) using combinations of keywords and Medical Subject Headings (MeSH) terms related to surgical outreach, global surgery, trauma epidemiology, facial plastic surgery, ethnic rhinoplasty, capacity building in LMICs, and health system strengthening.
Studies published between 2012 and 2024 were included, with a particular focus on literature from the past decade. In addition to indexed peer-reviewed articles, relevant reports from the World Health Organization (WHO), World Bank, and major surgical non-governmental organizations (NGOs) were reviewed to ensure comprehensive inclusion of both clinical and operational perspectives on global surgery.
Inclusion criteria comprised English-language publications addressing:
· Surgical access or reconstructive surgery in LMICs
· Trauma burden
· Outreach models (vertical, horizontal, diagonal)
· Cultural and ethnic considerations in facial plastic surgery
· Global health ethics, training, and authorship
· Use of telemedicine in surgical care
Exclusion criteria included:
· Studies focused exclusively on high-income countries
· Articles unrelated to surgical service delivery, access, or outreach
All retrieved records were screened in three stages:
1. Title screening to remove unrelated topics;
2. Abstract screening against inclusion/exclusion criteria;
3. Full-text review for final eligibility.
Reference lists were manually examined using a snowballing approach to identify additional relevant studies. Included articles were grouped thematically, and findings were synthesized narratively. The review followed best-practice guidance for narrative reviews and was informed by frameworks on ethical outreach, sustainability in global surgery, and health systems strengthening beyond the WHO’s six building blocks.
RESULTS
Six key domains of global surgery considerations were identified: workforce limitations, infrastructure gaps, economic and geographic barriers, training deficits, cultural considerations, and outreach models. These key domains and main findings are summarized in Table 1[1,6-16].
Summary of key domains and main findings in global surgery review
| Domain | Key challenges | Impact on reconstructive rhinoplasty |
| 1. Workforce limitations[7,8] | Fewer than 1 plastic surgeon per 100,000 population in sub-Saharan Africa; workforce concentrated in urban areas; otorhinolaryngology/facial plastic surgery often performed by general surgeons | Limited access in rural areas; reduced subspeciality expertise; compromised patient care |
| 2. Infrastructure gaps[6,8] | Limited operating theatre capacity; shortages of ICU beds; inconsistent anesthesia support; unreliable sterile supply chains | Limits feasibility of performing safe and complex procedures such as rhinoplasty |
| 3. Economic and geographic barriers[7,9,10] | Limited insurance cover for reconstructive surgery; out-of-pocket costs for patients; long travel distances to tertiary centres | Reduced surgical uptake; inequitable access; delayed presentation |
| 4. Training deficits[1,11] | Few regional rhinoplasty fellowships; limited exposure to advanced techniques; reliance on abroad training | Skill gaps; limited local mentorship; ongoing brain drain |
| 5. Cultural considerations[12,13] | Perception of cosmetic surgery as a luxury; cultural stigma around plastic surgery | Reduced acceptance even for medically indicated reconstruction |
| 6. Outreach models[11,14,15,16] | Vertical mission lacks sustainability; diagonal models integrate training and infrastructure; telemedicine supports follow-up | Sustainability depends on long-term partnerships and system strengthening |
Plastic surgery in resource-limited settings: the African context
Worldwide, facial plastic and reconstructive surgery is performed by ENT surgeons, general plastic surgeons, and oral and maxillofacial surgeons, depending on the regional context. The number of ENT specialists in Southern Africa is significantly lower at 0.18 clinicians per 100,000 population in comparison to the global average of 2.19 per 100,000 population; these shortages were significant in Zambia and Malawi[8]. Similarly, there is less than one plastic surgeon for every 100,000 individuals in Sub-Saharan Africa; in Zambia, there is 1 specialist plastic surgeon who provides care for the ~19 million population[7]. With limited availability of surgical sub-specialists, services are concentrated mainly in urban areas, leaving rural regions particularly underserviced[7,8]. Compounding the shortage of ENT and plastic surgery specialists, most of these countries are resource-restricted, with limited or no availability of equipment and medications[8]. It is estimated that only 11% of all patients who require plastic surgery treatment receive access to those services in these regions[7].
Outreach and international collaboration
NGOs and volunteer surgeons play a central role in addressing the unmet surgical needs in LMICs[11]. Outreach models were pioneered by Interplast, where teams from resource-rich countries delivered short-term reconstructive care in low-resource settings[14]. Globally, 131 reconstructive NGOs operate at 718 sites across 136 LMICs, with most activity in Africa and Asia[11].
Several models of international collaboration exist [Figure 1]. The traditional vertical model involves short, 1-4 week surgical missions focused on high-volume service delivery, often with minimal follow-up. This approach allows for rapid implementation but provides limited skills transfer and perpetuates dependence on external teams[1,17]. Horizontal and diagonal collaborative models have been developed for more sustainable engagement. Horizontal models are longer-term programs with sustained support, focusing on broader healthcare infrastructure changes[17]. A diagonal model focuses on a bidirectional relationship with integration into existing infrastructure, eventually allowing sustained service provision that combines surgical care with education, research development, and skills transfer[17]. Diagonal models aim to achieve self-sustaining revenue, infrastructure development, education and training, and skills transfer through long-term, sustained relationships[14,15].
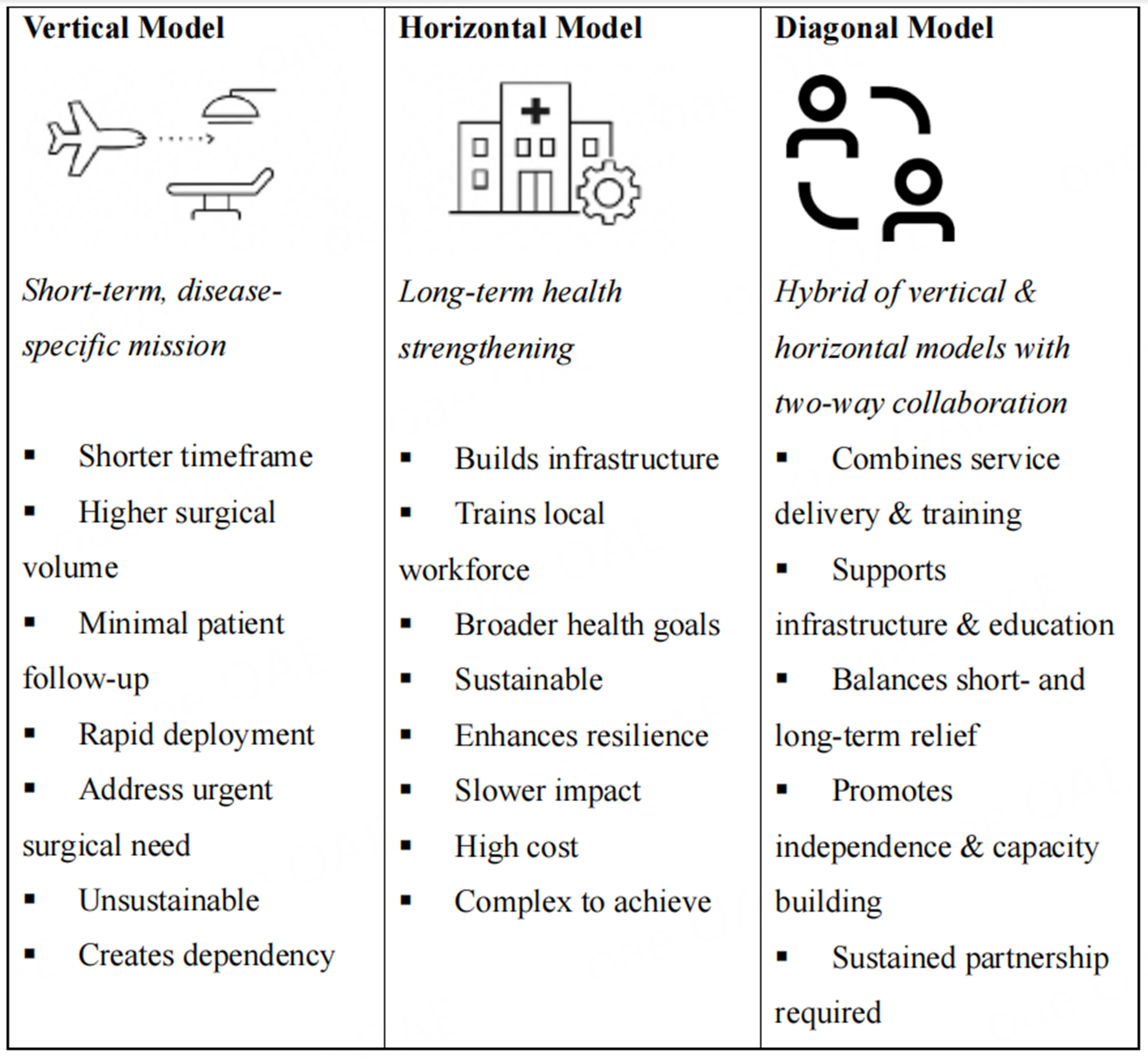
Figure 1. International outreach models.
Guidelines for sustainable global surgical care outline best practices for outreach collaborations[18-20]. These emphasize aligning outreach with local needs, training providers, monitoring outcomes, ensuring cost efficiency, and maintaining continuity with partner institutions[20]. Effective short-term missions require an understanding of local health system capacity, including infrastructure, workforce, perioperative resources, and drug availability[19,21]. Despite emerging protocols, most guidelines are authored by high-income partners, reflecting limited host country involvement in their development[22], further highlighting persistent inequities in collaboration, publication, and authorship[23,24].
Technology for capacity building
Clinical care
Telemedicine has become an important tool for extending surgical outreach in LMICs, helping overcome geographic, infrastructural, and workforce barriers that limit follow-up and continuity of care in traditional mission models[25].
A 2022 scoping review of 178 studies across 53 LMICs showed rapid growth in the use of simple telemedicine platforms such as mobile phones, video calls and WhatsApp. These methods were used for postoperative follow-up, patient education, and consultations[16]. These low-cost approaches have the potential to improve access and support remote clinical decision-making. However, it is important to note that additional research is needed, as the evidence base is limited; in this review, fewer than one-third of the studies met key quality criteria, and only 13% reported patient-centered outcomes[16]. While not a panacea, telemedicine extends specialist reach, enhances collaboration, and supports longitudinal care, making it a vital adjunct to global surgery.
Education development
With regard to surgical training opportunities, there are limited options available within LMICs. The majority of training programs, especially subspecialty training opportunities, are located in high-income countries, where accessibility and funding for surgeons from LMICs are limited. The need for trainees to travel internationally for training further exacerbates the shortage of surgeons serving these regions. According to the authors’ research, only five facial plastics training programs were identified in LMICs. While this may not be exhaustive, it highlights the dearth of in-country or in-region opportunities for skill advancement.
Tele-mentoring increasingly supports capacity building through remote surgical mentoring, simulation-based education, and continuing medical education (CME) for local providers[16,25]. However, challenges persist, including inadequate digital infrastructure, unreliable electricity, data security issues, and ethical or medicolegal uncertainties when surgical decisions are made across borders[16]. Effective integration requires investment in technology, training, and context-specific guidelines aligned with local health policies.
Culturally specific rhinoplasty
Aesthetics of global rhinoplasty
Much of the traditional rhinoplasty literature, technique development, and aesthetic definitions are centered on White patients of European descent[5]. However, patients from different ethnic backgrounds exhibit varied phenotypes and nuances in nasal anatomy. Applying the Caucasian aesthetic to a more diverse population can lead to outcomes that are discordant with both the patient’s cultural identity and individual aesthetic goals[5,26]. In the 21st century, there is clearly greater ethnic diversity among patients seeking rhinoplasty surgery[27]. Indeed, the term “ethnic rhinoplasty” to describe any non-Caucasian nasal surgery is increasingly seen as overly simplistic[28,29]. Additionally, there has been an overall shift in non-Caucasian patients’ aesthetic desires in rhinoplasty, focusing on improvements that preserve ethnic character[29].
In light of this, there has been increased attention to better defining the diversity of nasal anatomy globally. However, initial definitions of mesorrhine, platyrrhine, and leptorrhine nasal structures have failed to encompass the wider variations in presenting anatomy[30]. Overall, there has been an uptick in publications focusing on rhinoplasty surgery among diverse ethnic backgrounds [Table 2]. As part of this research effort on diverse nasal anatomy, a 2022 scoping review attempted to classify nasal anatomy presentations according to ethnic and regional variants[5]. Notably, although publications on both anatomic variation and techniques for culturally or ethnically preserving aesthetic outcomes are increasing, much of the literature is authored by researchers in high-income countries, with little to no representation from diverse authorship.
Summary of ethnic rhinoplasty findings from various studies
| Ethnic group | Key nasal features | Subtypes classifications | Surgical consideration | References |
| African/African American | Flat, wide dorsum; short nasal bones; thick sebaceous skin; bulbous tip; flared alae; low radix | African, Afro-Caucasian, Afro-Indian | Dorsal augmentation preferred over osteotomy; cartilage grafting for tip projection; alar base narrowing often needed | Momoh et al., Semin Plast Surg, 2009[31] |
| East Asian (e.g., Chinese, Korean, Japanese) | Short nose, low radix, wide dorsum, thick soft tissue envelope, weak alar cartilages, horizontal nostril orientation | Three subtypes based on lobule prominence, tip definition, dorsum slope | Tip and dorsum augmentation often needed; cartilage grafting essential due to weak structure | Patel and Most, Otolaryngol Clin N Am, 2020[32] |
| Middle Eastern | Dorsal hump, hanging columella, thick skin, soft cartilage, over-projected tip, wide dorsum | Not subtyped anatomically but culturally diverse | Common dissatisfaction with nasal tip and profile; patient satisfaction significantly improves post-op (FACE-Q) | Maassarani et al., Cureus, 2023[13] |
| Indian (South Asian) | North: long, narrow leptorrhine noses with greater projection South: Broadest nasal width, thicker skin, under-projected dorsum. Himalayan: Shorter, flatter noses with anteriorly directed nostrils. | North Indian and South Indian | Varies by regional subtype; Surgical strategy should be region-specific, respecting major morphological differences | Mehta and Srivastava, JPRAS, 2017[33] |
| Hispanic/Mestizo | Thick skin, short nasal bones, broad alar base, weak medial crura, low radix, pseudohumps Castilian, Mexican-American, Mestizo, Caribbean | Castilian, Mexican-American, Mestizo, Caribbean | Tip support and augmentation often required; classification guides strategy for dorsal/tip balance | Patel and Most, Otolaryngol Clin N Am, 2020[32] |
Hall et al. conclude that using broad racial and ethnic categories to describe nasal anatomy in rhinoplasty is ultimately problematic, as these classifications are based on outdated anthropological concepts and do not accurately reflect individual variability[34]. Instead, they propose a novel, anatomy-based classification system that categorizes nasal features into five distinct types based on objective measurements and observable anatomical characteristics, such as the support structure, dorsum shape, skin thickness, radix height, nasal length, and nostril shape[34] [Table 3]. The results demonstrate that this approach can facilitate more precise surgical interventions, improve communication between surgeon and patient, and promote inclusivity, potentially helping to reduce subconscious biases. An objective, anatomy-focused classification allows the surgeon to tailor procedures to the patient’s unique anatomy, thereby enhancing patient care and surgical outcomes[34].
Description of nasal types[34]
| Type | Key features |
| I | Weak support, thick sebaceous skin, wide dorsum, bulbous tip, under-projected, wide alar base |
| II | Low radix, wide bony vault, concave dorsum, bulbous tip, more horizontal nostrils |
| III | Moderate support, moderate skin, wide dorsum, bulbous, under-projected tip, variable nostril orientation |
| IV | Slightly stronger support, thick skin, prominent dorsum, variable tip and nostril shape |
| V | Strong support, supportive cartilage, straight to convex dorsum, mildly bulbous tip, vertically oriented nostrils |
Surgical considerations in global rhinoplasty
Establishing and achieving the functional and aesthetic goals of rhinoplasty surgery in non-Caucasian patients requires both an understanding of the range of nasal anatomy and elements of facial harmony[26,28,35]. An important consideration is that patients with higher Fitzpatrick scores are more prone to hypertrophic scarring or hyperpigmentation[26]. Additionally, in many non-Caucasian ethnic groups, the skin-soft-tissue envelope is not only thicker but also less pliant. Furthermore, there is a dominant fatty layer, most prominent over the lower lateral cartilages, which can complicate dissection and subsequent efforts at nasal tip definition. However, caution must be used when thinning the fatty layer to ensure the dermal plexus is not damaged, as this can lead to potential scarring or hyperpigmentation[26,28]. Finally, it is important to aggressively eliminate dead space after tip refinement to allow the refined tip to show through[26].
With regard to the structural elements of the nose, a wide array of structural maneuvers, grafting techniques, and grafting materials must be employed. In particular, the size and development of the nasal septum show wide variation across different backgrounds. In the non-Caucasian nose, there tends to be less septal cartilage available for grafting, thus requiring the use of other sources of cartilage, including rib and auricular cartilage[28]. Surgeons need to consider not only the time and skill required for autologous graft harvesting or the availability of allograft materials, but also the potentially increased risk of graft complications[26,36].
Implications for surgical outreach and skills transfer
The trauma burden in South Africa and delayed presentation - a case study
KwaZulu-Natal (KZN), a populous province in eastern South Africa, continues to experience a significant burden of trauma-related injuries, placing immense strain on its healthcare system. Over a 10-year period, 1,263,847 trauma-related visits to emergency departments were recorded across the province, reflecting the persistent and widespread nature of injury-related morbidity in the region. Zooming into a more focused setting, a two-year audit conducted in the municipality of Pietermaritzburg, a key urban and referral center in KZN, reported 10,644 trauma presentations across just three hospitals. Notably, 69.6% of these cases were due to blunt force trauma, underscoring the high prevalence of non-penetrating injuries in this community[9,10].
Nasal bone fractures, commonly caused by blunt trauma, can lead to lasting functional and aesthetic issues if left untreated. In resource-constrained settings such as KZN, limited reconstructive services result in long-term functional disability for untreated patients and further underscore the need for surgical outreach. This also highlights the role of longitudinal skills transfer and programmatic development to better serve these patient populations. Volunteer outreach surgeons must be familiar with local cultural norms and expectations, and consider ethnic surgical differences related to both anatomy and aesthetic goals. As baseline anatomy varies among patients of different ethnic backgrounds, an understanding of anatomic variance and the need for a range of surgical techniques to address functional and aesthetic concerns is critical. Additionally, collaboration across the various specialties that treat these injuries, combined with awareness of baseline surgical knowledge and available surgical tools, is essential for program longevity.
DISCUSSION
Global rhinoplasty
Reconstructive rhinoplasty in LMICs represents a critical yet under-resourced surgical need. It is a procedure essential to restoring both form and function in patients with congenital or acquired deformities. Gaps include limited access to affordable surgical treatment due to limited workforce and resources[11], as well as limitations in access to surgical skill expansion and training opportunities. An American-based institution that offers an international observership program concluded that surgical trainees from LMICs can benefit from international rotations through both direct knowledge transfer and ongoing knowledge-sharing initiatives[37]. There is a clear need for international outreach, capacity building, and tele-mentoring, all of which have the potential to significantly improve access to care and patient outcomes[1,2,16,18,38].
Specifically related to culturally specific rhinoplasty, there has been increasing attention to and appreciation of ethnic variance in nasal anatomy, breadth of patient aesthetic and functional goals, and range of techniques in addressing these goals. The nose is a highly individualized structure shaped by genetics and the environment; thus, there are important implications for graft choice, surgical technique, and aesthetic expectations across diverse populations[5]. Functional considerations must remain paramount, especially where trauma-related deformities predominate, as highlighted by the high burden of blunt trauma in KZN[6]. Despite promising advances, significant gaps remain. Resource constraints such as graft materials and instrumentation shortages necessitate innovative adaptations, including autologous graft harvesting and procedural prioritization frameworks. Additionally, postoperative care and complication management require local protocols tailored to limited antibiotic availability and follow-up challenges[16,25].
Outreach systems
The WHO Health System Building Blocks Framework, introduced in 2007, outlines six essential and interrelated components necessary for a well-functioning health system: (1) service delivery; (2) health workforce; (3) health information systems; (4) access to essential medicines and technologies; (5) financing; and (6) leadership and governance. This model provides a structured lens through which health system performance and gaps can be assessed, particularly in LMICs where systems are often fragmented and/or under-resourced. In the context of global surgical outreach, these building blocks are critical for evaluating not only the clinical impact of interventions, but also their sustainability, scalability, and alignment with national health priorities[39].
Outreach models that fail to address all six components risk delivering temporary solutions rather than building long-term capacity; conversely, programs grounded in this framework, particularly those aligned with diagonal approaches, are more likely to promote system-wide strengthening and equitable access to surgical care[39].
In the limited data available regarding outreach efforts, most studies primarily describe the positive experiences of resource-rich participants but provide little information about the experiences of the receiving stakeholders[40]. A scoping review by Velin et al. highlighted the challenges faced by some receiving teams, including poor post-surgical follow-up, limited knowledge transfer, concerns about ethics and equity, and administrative and financial issues[40]. Additionally, continued assistance by NGOs can relieve pressure on governments to provide these services. A notable and impactful quote from this article states: “the groups were not very interested in teaching either, because they needed to do numbers. Numbers to be able to bring to their sponsors and to say to them: ‘I operated on 50 children in ten days’, instead of saying to them, ‘I operated on five and I taught a surgeon’.” This underscores the mixed impact and competing goals of visiting missions[40].
Upskilling local providers
Elective reconstructive rhinoplasty in LMICs hinges on building local capabilities. The surgical education adage “see one, do one, teach one” should be expanded to system-wide skill dissemination with the goal of upskilling and fostering collaborative surgical initiatives. The updated goal could be stated as: “see one, do one, teach one, expand surgical boundaries together”. Upskilling can include hands-on visiting workshops, formal short-term fellowship rotations, and educational opportunities not only for clinical skills but also for formal teaching and leadership development. A summary of suggested recommendations is provided in Table 4.
Authors’ suggestions and rationale for expanding global rhinoplasty
| Suggestions | Rational |
| 1. Combine short-term missions with long-term local training | Provide short-term mission immediate surgical relief, but must be embedded within programs that build local surgical capacity, ensuring sustainability |
| 2. Standardized protocols while tailoring to local context | Use existing global guidelines but adapt them based on host-country realities, such as drug availability and perioperative care infrastructure |
| 3. Strengthen partnerships & promote host-country leadership | Shift from donor-led missions to collaborative models where local providers co-design and lead surgical intervention, ensuring relevance & ownership |
| 4. Blend local & international missions to transition responsibility | Organizations such as Operation Smile show how international missions can evolve into local missions as local surgeons are trained and equipped |
| 5. Ensure service delivery is paired with system inputs | Avoid offering only surgeries, support should include equipment, medication supply chains, and maintenance training to ensure lasting impact |
| 6. Measure outcomes alongside equity & ethics | Use DALYs and surgical indicators to evaluate impact, but also assess ethical parameters, such as patient consent, cultural respect, and equitable access |
| 7. Share authorship and credit with local stakeholders | Scientific publications & guidelines should include local co-authors & perspectives to prevent knowledge colonialism & ensure credibility |
| 8. Expand follow-up systems alongside mission planning | Outreach teams must create referral pathways & telehealth options to track complications & ensure longitudinal patient care |
Digital technologies have emerged as invaluable adjuncts. Tele-mentoring bridges geographic divides, enabling local surgeons to manage complex reconstructions under expert guidance while fostering confidence and independence. Platforms enabling asynchronous learning, live virtual operating room participation, and peer-to-peer case discussions further support ongoing education and quality assurance[1,16,25].
CONCLUSIONS
There is a growing recognition that access to broad reconstructive surgical services is critical for serving a global population. Ethnically diverse rhinoplasty anatomy, aesthetic goals, and surgical techniques require greater elucidation, with specific attention to globally diverse authorship.
Visiting surgeons play an important role, not only in performing operations but also in training local teams, introducing new clinical skills, and building sustainable systems. However, impact is maximized only when these efforts are ethically grounded and designed for long-term integration with local healthcare structures. It is critical to collect and evaluate longitudinal clinical outcomes for different outreach models, as well as the effect of capacity building. Promoting local leadership in collaborations and supporting sustainable financing is central to ethical, long-term partnerships. Finally, a longitudinal relationship allows for continuity of care for complex patients or those who may require revision surgery.
The authors, representing both LMIC and high-income perspectives, emphasize that strengthening reconstructive rhinoplasty services is not just about surgical technique but about building resilient, self-sufficient health systems through equitable partnerships.
DECLARATIONS
Authors’ contributions
Made substantial contributions to the conception and design of the review, and performed literature search and synthesis: Maistry S, Toman J
Provided administrative, technical, and material support: Toman J
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
ChatGPT was used to assist with preparation of the Graphical Abstract and elements of Figure 1.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Ullrich PJ, Ramsey MD. Global plastic surgery: a review of the field and a call for virtual training in low- and middle-income countries. Plast Surg. 2023;31:118-25.
2. Goettke E, Coultas C, White M, Leather AJM. Conceptualising sustainability in the surgical work of non-governmental organisations in low and middle-income countries : a scoping review protocol. BMJ Open. 2021;11:e048046.
3. Holmer H, Lantz A, Kunjumen T, et al. Global distribution of surgeons, anaesthesiologists, and obstetricians. Lancet Glob Health. 2015;3:S9-11.
4. Tasman AJ. Rhinoplasty - indications and techniques. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2007;6:Doc09.
5. Heiman AJ, Nair L, Kanth A, Baltodano P, Patel A, Ricci JA. Defining regional variation in nasal anatomy to guide ethnic rhinoplasty: a systematic review. J Plast Reconstr Aesthet Surg. 2022;75:2784-95.
6. Tefera A, Lutge EE, Moodley N, et al. Tracking the trauma epidemic in KwaZulu-Natal, South Africa. World J Surg. 2023;47:1940-5.
7. Mugisha N, Uwishema O, Noureddine R, et al. Access to specialist plastic surgery in rural vs. Urban areas of Africa. BMC Surg. 2024;24:418.
8. Lukama L, Aldous C, Kuhn W, Michelo C, Kalinda C. Ten years of ear, nose and throat (ENT) services in Southern Africa: a scoping review. Glob Health Action. 2024;17:2370102.
9. Moodley NB, Aldous C, Clarke DL. An audit of trauma-related mortality in a provincial capital in South Africa. S Afr J Surg. 2014;52:101-4.
10. Moodley NB, Clarke DL, Aldous C. Current trauma patterns in Pietermaritzburg. S Afr J Surg. 2015;53:42-44.
11. Chao AH, McAllister JR. Reconstructive surgery outreach to low- and middle-income countries: an interdisciplinary analysis of 131 non-governmental organizations. J Glob Health. 2022;12:04002.
12. Pozzi M, Fàdel C, Bolletta A, Cuomo R, Roxo CW. Ethnic rhinoplasty: preliminary results of our technique in the pursuit of the harmonious nose. J Plast Reconstr Aesthet Surg. 2023;87:135-46.
13. Maassarani D, Challita R, Zeaiter N, et al. Ethnic rhinoplasty: a middle east-centered patient satisfaction survey using the FACE-Q questionnaire. Cureus. 2023;15:e40048.
14. Nagengast ES, Munabi NCO, Xepoleas M, Auslander A, Magee WP 3rd , Chong D. The local mission: improving access to surgical care in middle-income countries. World J Surg. 2021;45:962-9.
15. Patel PB, Hoyler M, Maine R, Hughes CD, Hagander L, Meara JG. An opportunity for diagonal development in global surgery: cleft lip and palate care in resource-limited settings. Plast Surg Int. 2012;2012:892437.
16. Owolabi EO, Mac Quene T, Louw J, Davies JI, Chu KM. Telemedicine in surgical care in low- and middle-income countries: a scoping review. World J Surg. 2022;46:1855-69.
17. Leversedge C, McCullough M, Appiani LMC, Đình MP, Kamal RN, Shapiro LM. Capacity building during short-term surgical outreach trips: a review of what guidelines exist. World J Surg. 2023;47:50-60.
18. Caldron PH, Impens A, Pavlova M, Groot W. A systematic review of social, economic and diplomatic aspects of short-term medical missions. BMC Health Serv Res. 2015;15:380.
19. Butler M, Drum E, Evans FM, et al. Guidelines and checklists for short-term missions in global pediatric surgery: recommendations from the American Academy of Pediatrics Delivery of Surgical Care Global Health Subcommittee, American Pediatric Surgical Association Global Pediatric Surgery Committee, Society for Pediatric Anesthesia Committee on International Education and Service, and American Pediatric Surgical Nurses Association, Inc. Global Health Special Interest Group. J Pediatr Surg. 2018;53:828-36.
20. Grimes CE, Maraka J, Kingsnorth AN, Darko R, Samkange CA, Lane RH. Guidelines for surgeons on establishing projects in low-income countries. World J Surg. 2013;37:1203-7.
21. Roche SD, Ketheeswaran P, Wirtz VJ. International short-term medical missions: a systematic review of recommended practices. Int J Public Health. 2017;62:31-42.
22. Lasker JN, Aldrink M, Balasubramaniam R, et al. Guidelines for responsible short-term global health activities: developing common principles. Global Health. 2018;14:18.
23. Nyangulu WJ. Global health collaborative research: beyond mandatory collaboration to mandatory authorship. Glob Health Res Policy. 2023;8:48.
24. Smith E, Hunt M, Master Z. Authorship ethics in global health research partnerships between researchers from low or middle income countries and high income countries. BMC Med Ethics. 2014;15:42.
25. Mehta A, Andrew Awuah W, Tunde Aborode A, et al. Telesurgery’s potential role in improving surgical access in Africa. Ann Med Surg. 2022;82:104511.
28. Kim DW, Hwang HS. Traumatic rhinoplasty in the non-Caucasian nose. Facial Plast Surg Clin North Am. 2010;18:141-51.
30. Eggerstedt M, Rhee J, Buranosky M, et al. Nasal skin and soft tissue thickness variation among differing races and ethnicities: an objective radiographic analysis. Facial Plast Surg Aesthet Med. 2020;22:188-94.
31. Momoh AO, Hatef DA, Griffin A, Brissett AE. Rhinoplasty: the african american patient. Semin Plast Surg. 2009;23:223-31.
32. Patel PN, Most SP. Concepts of facial aesthetics when considering ethnic rhinoplasty. Otolaryngol Clin North Am. 2020;53:195-208.
33. Mehta N, Srivastava RK. The Indian nose: an anthropometric analysis. J Plast Reconstr Aesthet Surg. 2017;70:1472-82.
34. Hall DB, McColl LF, Katta J, Bonanno J, Kim LR, Nesemeier BR. Bringing inclusivity to “ethnic” rhinoplasty: a novel anatomical classification system. Facial Plast Surg Aesthet Med. 2025;27:61-5.
35. Szychta P, Rykała J, Kruk-Jeromin J. Individual and ethnic aspects of preoperative planning for posttraumatic rhinoplasty. Eur J Plast Surg. 2011;34:245-9.
36. Hudise JY, Aldhabaan SA, Aldosari BF. Complications of the nasal dorsum reconstruction using autologous or alloplastic grafts: evidence from systematic review and meta-analysis. Braz J Otorhinolaryngol. 2022;88:406-20.
37. Valencia-Rojas N, Aboutanos MB, Rodas EB. Fostering knowledge transfer to strengthen the surgical workforce in LMIC: lessons learned from an international observership program. Panam J Trauma Crit Care Emerg Surg. 2021;10:61-5.
38. Martiniuk AL, Manouchehrian M, Negin JA, Zwi AB. Brain gains: a literature review of medical missions to low and middle-income countries. BMC Health Serv Res. 2012;12:134.
39. Sacks E, Morrow M, Story WT, et al. Beyond the building blocks: integrating community roles into health systems frameworks to achieve health for all. BMJ Glob Health. 2018;3:e001384.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.