


Perspectives of Professor Barry A. Franklin: no pill can enhance fitness
 0
0 Abstract
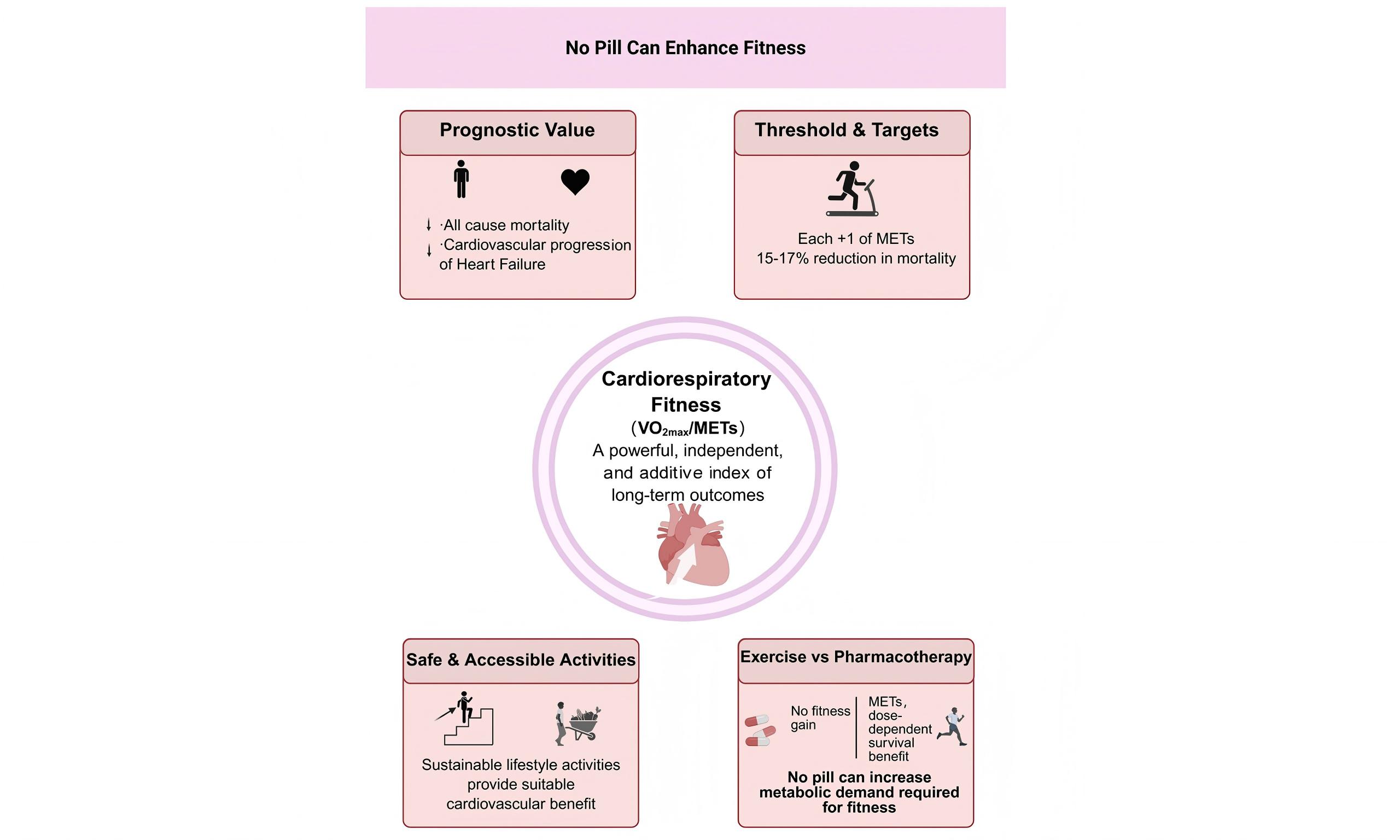
In this special interview, Professor Barry A. Franklin shared key experiential and research-based insights on professional success, exercise-based cardiovascular therapy, and the impactful role of cardiorespiratory fitness in promoting long-term health outcomes. (a) Professional success is built on clearly defined written goals, consistent daily action, personal responsibility, a mindset of happiness, optimism, and gratitude, and exemplary service to others; (b) Outstanding academic and clinical careers require effective mentorship, strong communication skills, advanced training and continuing education, disciplined work habits, and proactive management of stress and health; (c) Aerobic and resistance training provide complementary benefits in combating cardiovascular disease, with aerobic exercise contributing most strongly to long-term survival; (d) Cardiorespiratory fitness or VO2max (maximum volume of oxygen uptake), expressed as metabolic equivalents (METs), is a powerful, independent, and additive predictor of survival, with each 1-MET (one metabolic equivalent) increase associated with a mortality reduction of ~ 15%-17%; (e) Higher fitness levels significantly reduce the risk and improve the prognosis of heart failure with preserved ejection fraction and heart failure with reduced ejection fraction, independent of body mass index and traditional risk factors; (f) Although aerobic fitness declines rapidly with detraining, it is reversible, while muscle strength can be largely maintained with one resistance training session per week; (g) To date, no pharmacologic therapy can elicit the increases in metabolism needed to improve fitness, as well as the associated favorable adaptations, and safe, accessible activities such as stair climbing and daily walking provide substantial cardiovascular risk reduction.
Keywords
FOREWORD
Professor Barry A. Franklin, PhD, is a world leader in preventive cardiology and cardiac rehabilitation, with decades of experience spanning clinical practice, research, and education. He has served as president of the American Association of Cardiovascular and Pulmonary Rehabilitation and the American College of Sports Medicine and has authored over 700 scientific publications. Drawing on his distinguished career, Professor Franklin shared profound insights into personal growth and professional success, emphasizing the key role of setting clear goals and taking daily actions to achieve them.
In this interview, he further discussed, from an evidence-based perspective, the distinct roles of aerobic and resistance training in cardiac rehabilitation, highlighting their independent and additive contributions to improving long-term health outcomes in patients with coronary artery disease, heart failure, and hypertension. Additionally, Professor Franklin provided guidance for the development of young scholars and clinicians, including stress management, maintaining physical and mental well-being, and the importance of regular moderate-to-vigorous exercise and improved cardiorespiratory fitness for the prevention and rehabilitation of cardiovascular disease.
Q1: Looking back on your scientific career - one that has consistently placed you among the “Top 2% of Global Scientists” - what personal principles, work habits, and professional philosophies have most shaped your success? What lessons from your journey do you believe are most valuable for young investigators hoping to build a meaningful research career?
Prof. Franklin: Over the past four decades, one of my passions has been the study of highly successful people in all walks of life. I have learned that success does not happen by chance - it is created by setting specific daily and long-term written goals and taking consistent action every day to achieve them. In so many ways, our daily thoughts and actions create our future. Accordingly, you are your own fortune cookie.
From my observations, truly successful people tend to embrace and radiate three key traits: they are happy, optimistic, and deeply grateful. Beyond mindset, there are several principles that consistently precede major achievements and success across all fields. First, you must genuinely love what you do. Second, we largely create our own luck - about 90%-95% of outcomes in life are shaped by our thoughts and actions. Third, I encourage young people to take 100% responsibility for their lives rather than blaming others. I love the quote by the American painter, William H. Johnsen: “If it is to be, it is up to me”. Finally, focus on helping and admirably serving others which invariably brings rewards back in unexpected ways.
For young investigators, I offer five practical self-help strategies: secure a great mentor or mentors; continuously improve your communication skills through reading, writing, and speaking; pursue advanced degrees and additional training to build and strengthen your professional armamentarium; develop disciplined habits such as collaborating with others and rising very early to prioritize important work; and, ultimately, dedicate your professional career to a cause greater than yourself.
Q2: As someone who works closely with early-career clinicians and researchers, how do you help young colleagues manage stress and deadlines, maintain well-being, and protect their cardiovascular health while striving for academic excellence? Have you found any particularly effective strategies for supporting sustainable long-term health and career advancement?
Prof. Franklin: When you reach the top of the mountain, don’t forget to turn around and help those still climbing behind you. I was enormously helped by several mentors throughout my career, so I try to make myself available to young scholars - generously giving them the time they need for guidance, both professionally and personally. Helping students and junior colleagues is a core value I strongly believe in. If you want a long and sustainable career, you must also maintain and take opportunities to enhance your health and well-being. That means managing stress rather than reacting to it, eating a healthy diet rich in fruits, vegetables, whole grains, and seafood, getting adequate sleep, staying physically active, and avoiding cigarette smoking and drugs that may be addictive. Knowing your key health numbers - such as blood pressure, blood glucose, and cholesterol - is essential for long-term well-being. Professionally, I encourage young scholars to work on their goals every day instead of relying on occasional intense efforts. Daily consistency matters more than weekend overload. Get involved in professional organizations, increase your visibility by writing and speaking more, as well as doing committee work, and understand that setbacks and rejections line the road to success. Finally, periodically take time off. Regular breaks and brief vacations allow you to return refreshed and thinking more clearly, which ultimately leads to increased productivity.
Q3: In your research on exercise-based cardiovascular therapy, what differences have you observed between aerobics, resistance, and combined training in improving long-term health outcomes for patients with coronary artery disease, heart failure, or hypertension? When evaluating the effectiveness of exercise interventions, which physiological markers or biomarkers do you consider most informative? How do these data help clinicians tailor and adjust exercise prescriptions over time?
Prof. Franklin: Aerobic and resistance training are complementary forms of exercise, each providing independent and additive benefits. For patients with coronary artery disease, heart failure, or hypertension, I generally recommend a physical conditioning regimen involving both types of exercise. However, in patients with hypertension, resistance training should involve lighter weights with slightly more repetitions per set (i.e., 10-15)[1].
Although both aerobic and resistance training are associated with reduced mortality, aerobic training is clearly more important for long-term survival. Based on decades of research, I recommend that approximately 75%-80% of total training time be devoted to aerobic exercise, with the remaining 20%-25% focused on resistance training[2]. Complementary resistance training is often underappreciated, as it improves selected cardiovascular risk factors and reduces the rate-pressure product, lowering cardiac demand during lifting or carrying objects[3].
Cardiorespiratory fitness or VO2max, expressed as peak or maximal metabolic equivalents (METs), is one of the strongest predictors of mortality. Unfit individuals generally have two to three times higher mortality than fit individuals with comparable age and risk factor profiles. In patients with heart failure, higher fitness levels are consistently associated with better survival. Most epidemiologic studies show that each 1-MET (one metabolic equivalent) increase in exercise capacity is associated with a 15%-17% decrease in mortality[4].
When monitoring exercise interventions, I focus on simple but informative physiological markers, including resting heart rate, resting blood pressure, VO2max or cardiorespiratory fitness, and grip strength[5,6]. In general, lower resting heart rate and blood pressure indicate better prognosis. Improvements in these markers can help clinicians individualize and refine exercise prescriptions over time.
Q4: Heart failure with preserved ejection fraction (HFpEF) has become a major frontier in current heart failure research, with particular emphasis on pharmacologic therapies in recent years. From the perspective of exercise training and cardiac rehabilitation, are there any special considerations or recommendations for patients with HFpEF? In addition, are there notable differences in exercise evaluation between HFpEF and heart failure patients with reduced ejection fraction?
Prof. Franklin: In one of our previous studies, using the U.S. Veterans Administration database, we examined the relationship between cardiorespiratory fitness (peak METs) and the incidence of heart failure with preserved ejection fraction (HFpEF). We found a clear dose-response relationship: higher fitness levels, or improvements in fitness over time, were associated with a lower risk of developing HFpEF, independent of traditional heart failure risk factors and regardless of age, race, or sex. The take-home message is that moderate-to-vigorous physical activity and increased levels of cardiorespiratory fitness should be actively promoted to reduce HFpEF risk[3,7].
In another study, published in the European Journal of Heart Failure in 2019, we followed ~20,000 Veterans (men and women) for ~13 years, during which 2,979 heart failure events occurred[8]. We examined baseline VO2 and BMI. Regardless of body weight category - normal weight, overweight, or obese - low-fit individuals were 2.5-3.5 times more likely to develop heart failure (both preserved and reduced ejection fraction). These findings indicate that a low fitness level is a stronger predictor of heart failure risk than BMI, particularly when fitness ~ only 4.5 METs. Furthermore, our data suggested that to decrease the incidence of heart failure, it is better to be overweight or obese and fit than normal weight and unfit.
In our third publication, a Circulation scientific statement in 2023, we evaluated supervised exercise therapy in HFpEF[9]. We concluded that supervised exercise therapy elicits comparable or even greater improvements in exercise capacity and quality of life in HFpEF patients compared with those with reduced ejection fraction. From a clinical standpoint, this strongly supports expanding insurance reimbursement in the U.S. to include both heart failure phenotypes, not just reduced ejection fraction.
Overall, my conclusions are straightforward. Physical activity and cardiorespiratory fitness are underappreciated therapeutic tools for preventing heart failure and improving prognosis. Progressive, moderate-to-vigorous exercise is safe in patients with both preserved and reduced ejection fractions. Finally, an important initial goal for heart failure patients is achieving an exercise capacity > 5 METs, which substantially improves survival. This can be achieved when patients train at ≥ 3 METs[10]. Regular exercise training and improved fitness deserve recognition as core components (or objectives) of a comprehensive heart failure treatment regimen.
Q5: There are studies showing that improved cardiorespiratory fitness reduces the risk of cardiovascular disease, but the long-term effects of exercise interventions should be emphasized. Given your experience, after completing a medically supervised exercise program - for example, 12 weeks of aerobic training - how long do the cardioprotective effects persist if patients discontinue regular exercise? In clinical practice, how do you motivate patients to sustain long-term physical activity and monitor their fitness levels regularly? Additionally, can changes in VO2max or other cardiopulmonary indicators help to quantify prognosis and improvement, and how are these metrics incorporated into treatment or rehabilitation decisions?
Prof. Franklin: When aerobic training is discontinued, cardiorespiratory endurance declines much faster than muscle strength, with VO2max and MET capacity showing particularly rapid reductions[11-13]. A classic study demonstrated that just 3 weeks of bed rest resulted in a ~25% decline in VO2max, a loss comparable to that typically observed over three decades of aging. Importantly, this decline is largely reversible, as aerobic capacity can be restored to baseline within 2-3 weeks once exercise training is resumed[14,15]. Clinically, early mobilization strategies - such as frequent sitting and/or standing that provide transient orthostatic and gravitational stress - can substantially attenuate deconditioning in hospitalized cardiac patients.
In contrast, muscle strength is more resistant to detraining. Even when resistance training is reduced, just one training session per week is sufficient to maintain ~90%-95% of muscle mass and strength. Moreover, for most patients, a single set of 10-15 repetitions across multiple exercises achieves nearly 90% of the benefits of multiple-sets resistance training, making it a highly efficient intervention outside of athletic populations.
Regular physical activity provides mortality-reducing benefits comparable to major cardioprotective medications, such as aspirin, statins, beta-blockers, and ACE inhibitors, each of which typically reduces mortality by ~20%-25%[16-18]. In parallel, each 1-MET increase in exercise capacity is associated with a ~15%-17% reduction in mortality, whereas a 2-MET improvement corresponds to a ~30%-34% decrease in death risk. Exercise training should be viewed not as a replacement for pharmacotherapy, but as a critical complementary intervention that should be maintained over the long term. I tell our cardiac patients - you wouldn’t stop taking your prescribed cardioprotective medications, so don’t stop exercising! Why? Because exercise is medicine.
Finally, improvements in exercise capacity (VO2max or peak METs) have a strong and consistent impact on prognosis. Large cohort studies show that each incremental increase in fitness is associated with lower mortality, whereas declining fitness predicts worse outcomes across cardiovascular disease, stroke, dementia, and other conditions. Collectively, these findings underscore cardiorespiratory fitness as one of the most powerful and modifiable prognostic indicators in medicine and justify its primary role in guiding rehabilitation and long-term treatment decisions[4,19-21].
Q6: For many people, it is quite difficult to maintain a routine of daily exercise. Are there any alternative approaches, such as pharmacologic options, or would engaging in high-intensity exercise just once a week still be effective?
Prof. Franklin: This may sound surprising, but based on my 50 years of clinical experience, I am unaware of any pharmacologic therapy that can elicit the increase in VO2 or aerobic requirements needed for true cardiovascular conditioning. Appreciably raising the heart rate - whether through drugs, sauna use, or emotional stress - does not improve fitness. The true training stimulus is increasing somatic oxygen consumption, transitioning from 1 (resting) to 3-5 METs or more, and no drug can achieve this increase in metabolic rate[22-24].
High-intensity interval training (HIIT) can improve fitness in an accelerated manner, but the average additional gain in VO2max, relative to moderate intensity continuous training, is modest - about ~0.5 MET. What concerns me is safety. HIIT generally increases heart rates to 90%-95% of maximal, essentially mimicking a maximal treadmill or cycle ergometer exercise stress test. In cardiac patients, studies show a ~6-fold higher incidence of cardiac events with high-intensity training compared with moderate-intensity exercise. Given that ≥ 50% of individuals in their late 40 s and 50 s already have underlying coronary atherosclerosis, HIIT can trigger myocardial ischemia, threatening ventricular arrhythmias, or plaque rupture. Accordingly, outside of medically supervised settings, I do not believe it is prudent to recommend HIIT in this “at risk” population, with no data to suggest the potential added benefits outweigh the associated risks[25-27].
Instead, I recommend safer and more accessible alternatives with proven survival benefits. Regular stair climbing, as little as ≥ 5 flights per day, is associated with a 30%-35% reduction in mortality, as shown in large European cohorts and supported by earlier Harvard Alumni data. Likewise, daily walking provides substantial health benefits: 7,000-8,000 steps per day achieves near-maximal risk reduction across age and sex. Importantly, for habitually sedentary individuals, benefits begin at just 2,500-3,000 steps per day[28-31].
In short, before turning to unproven pharmacologic agents or unsupervised HIIT - especially in middle-aged and older adults (who likely have underlying atherosclerotic cardiovascular disease) - I strongly favor simple, safe, and readily accessible physical activity that reliably improves fitness and reduces mortality.
Q7: Your pioneering work in preventive cardiovascular exercise interventions and behavioral science - along with your recent book, GPS for Success: Skills, Strategies, and Secrets of Super, Achievers (Productivity Press, NY, NY, 2022), highlights the common traits shared by high achievers across all fields. When translating scientific evidence into daily practices for personal and professional growth, what important details or pitfalls do people tend to overlook? Which habits or mindsets are often underestimated, yet crucial for long-term success?
Prof. Franklin: If I had to concisely summarize key success principles from my research and experience, it would start with this: set your goals in writing and take action every day to achieve them. Goals that are not written down remain elusive. Perhaps Sir John Hargrave summed it up best when he said: “Until it’s on paper, it’s vapor”. Writing down your goals documents a commitment, and taking daily action is what ultimately brings them to fruition. The universe rewards action - not deciding, planning, or thinking about doing something.
I also emphasize prioritization. Do the most important work first, ideally very early in the morning, before distractions and fatigue occur - while your competitors are still sleeping. Progress comes from consistently working on what matters most, not from performing less important tasks. At the same time, young scholars should constantly seek opportunities and not fear rejection. Many doors open simply because someone is willing to ask. Recognize that rejection or setbacks regularly line the road to success.
Long-term success also requires a commitment to continuous self-improvement. Being just a little better than your competition - through publications, presentations, certifications, or newly acquired skills - can make a substantial difference over time. Collaboration is equally critical: people with complementary skill sets, working together on a common goal, can double, triple, and even quadruple their productivity. It’s the ultimate thrill ride! Effective time management amplifies this process, especially by using small blocks of time productively rather than letting them slip away. Perhaps Henry Ford summed it up best when he said: “It has been my observation that most people get ahead during the time that others waste”.
Finally, productivity increases when distractions are minimized. Eliminating time-wasting activities (e.g., watching television, endlessly surfing the internet, or running non-essential errands) and focusing your energy on meaningful projects can dramatically expand what you are able to accomplish. Small, consistent improvements, sustained over time, are what ultimately separate good careers from truly exceptional ones. By embracing the aforementioned skills, strategies, and proven principles, good luck will be increasingly attracted to you. It will happen. It cannot be otherwise. You are your own fortune cookie…
DECLARATIONS
Authors’ contributions
Lead the interview: Zhang Y, Franklin BA
Contributed to data interpretation and provided critical revision of the manuscript for important intellectual content: Zhang Y, Franklin BA, Li H
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This work was supported by the National Key Research and Development Program of China (2023YFC3606500, 2023YFC2506500, 2023YFC2506505), the Shanghai Clinical Research Center for Interventional Medicine (19MC1910300), the Special Clinical Research Project of the Shanghai Municipal Health Commission (20244Y0022), and the Shanghai “Rising Stars of Medical Talent” Youth Development Program [SHWSRS(2024)070].
Conflicts of interest
Franklin BA is an Editorial Board Member of the journal Vessel Plus. Zhang Y is a Youth Editorial Board Member of the journal Vessel Plus. Franklin BA and Zhang Y were not involved in any steps of the editorial process, including reviewer selection, manuscript handling, or decision-making. Li H declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Franklin BA, Eijsvogels TMH, Pandey A, Quindry J, Toth PP. Physical activity, cardiorespiratory fitness, and cardiovascular health: a clinical practice statement of the ASPC Part I: bioenergetics, contemporary physical activity recommendations, benefits, risks, extreme exercise regimens, potential maladaptations. Am J Prev Cardiol. 2022;12:100424.
2. Paluch AE, Boyer WR, Franklin BA, et al. Resistance exercise training in individuals with and without cardiovascular disease: 2023 update: a scientific statement from the American Heart Association. Circulation. 2024;149:e217-31.
3. Franklin BA, Eijsvogels TMH, Pandey A, Quindry J, Toth PP. Physical activity, cardiorespiratory fitness, and cardiovascular health: a clinical practice statement of the American Society for Preventive Cardiology Part II: Physical activity, cardiorespiratory fitness, minimum and goal intensities for exercise training, prescriptive methods, and special patient populations. Am J Prev Cardiol. 2022;12:100425.
4. Franklin BA, Quindry J. High level physical activity in cardiac rehabilitation: implications for exercise training and leisure-time pursuits. Prog Cardiovasc Dis. 2022;70:22-32.
5. Harber MP, Kaminsky LA, Arena R, et al. Impact of cardiorespiratory fitness on all-cause and disease-specific mortality: advances since 2009. Prog Cardiovasc Dis. 2017;60:11-20.
6. Franklin BA, Wedig IJ, Sallis RE, Lavie CJ, Elmer SJ. Physical activity and cardiorespiratory fitness as modulators of health outcomes: a compelling research-based case presented to the medical community. Mayo Clin Proc. 2023;98:316-31.
7. Kokkinos P, Faselis C, Pittaras A, et al. Cardiorespiratory fitness and risk of heart failure with preserved ejection fraction. Eur J Heart Fail. 2024;26:1163-71.
8. Kokkinos P, Faselis C, Franklin B, et al. Cardiorespiratory fitness, body mass index and heart failure incidence. Eur J Heart Fail. 2019;21:436-44.
9. Sachdev V, Sharma K, Keteyian SJ, et al. Supervised exercise training for chronic heart failure with preserved ejection fraction: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2023;147:e699-715.
10. Franklin BA, Brinks J, Berra K, Lavie CJ, Gordon NF, Sperling LS. Using metabolic equivalents in clinical practice. Am J Cardiol. 2018;121:382-7.
11. Mujika I, Padilla S. Detraining: loss of training-induced physiological and performance adaptations. Part I: short term insufficient training stimulus. Sports Med. 2000;30:79-87.
12. Neufer PD. The effect of detraining and reduced training on the physiological adaptations to aerobic exercise training. Sports Med. 1989;8:302-20.
13. Lo MS, Lin LL, Yao WJ, Ma MC. Training and detraining effects of the resistance vs. endurance program on body composition, body size, and physical performance in young men. J Strength Cond Res. 2011;25:2246-54.
14. Lepers R, Mater A, Assadi H, Zanou N, Gremeaux V, Place N. Effect of 12 weeks of detraining and retraining on the cardiorespiratory fitness in a competitive master athlete: a case study. Front Physiol. 2024;15:1508642.
15. Zheng J, Pan T, Jiang Y, Shen Y. Effects of short- and long-term detraining on maximal oxygen uptake in athletes: a systematic review and meta-analysis. Biomed Res Int. 2022;2022:2130993.
16. Sheppard JP. Should exercise be considered as an alternative to drug treatment in patients with low-risk mild hypertension? Br J Sports Med. 2019;53:848-9.
17. Naci H, Ioannidis JP. Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study. BMJ. 2013;347:f5577.
18. Kunutsor SK, Laukkanen JA. Physical activity, exercise and adverse cardiovascular outcomes in individuals with pre-existing cardiovascular disease: a narrative review. Expert Rev Cardiovasc Ther. 2024;22:91-101.
19. Martin BJ, Arena R, Haykowsky M, et al. Cardiovascular fitness and mortality after contemporary cardiac rehabilitation. Mayo Clin Proc. 2013;88:455-63.
20. Franklin BA, Lavie CJ, Squires RW, Milani RV. Exercise-based cardiac rehabilitation and improvements in cardiorespiratory fitness: implications regarding patient benefit. Mayo Clin Proc. 2013;88:431-7.
21. Franklin BA, McCullough PA. Cardiorespiratory fitness: an independent and additive marker of risk stratification and health outcomes. Mayo Clin Proc. 2009;84:776-9.
22. Azócar-Gallardo J, Ojeda-Aravena A, Báez-San Martín E, et al. Effect of a concurrent training program with and without metformin treatment on metabolic markers and cardiorespiratory fitness in individuals with insulin resistance: a retrospective analysis. Biomolecules. 2024;14:1470.
23. Crowley E, Powell C, Carson BP, Davies RW. The effect of exercise training intensity on VO2max in healthy adults: an overview of systematic reviews and meta-analyses. Transl Sports Med. 2022;2022:9310710.
24. Belanger MJ, Rao P, Robbins JM. Exercise, Physical activity, and cardiometabolic health: pathophysiologic insights. Cardiol Rev. 2022;30:134-44.
25. McGregor G, Powell R, Begg B, et al. High-intensity interval training in cardiac rehabilitation: a multi-centre randomized controlled trial. Eur J Prev Cardiol. 2023;30:745-55.
26. Kristiansen J, Sjúrðarson T, Grove EL, et al. Feasibility and impact of whole-body high-intensity interval training in patients with stable coronary artery disease: a randomised controlled trial. Sci Rep. 2022;12:17295.
27. Milani JGPO, Milani M, Verboven K, Cipriano G Jr, Hansen D. Exercise intensity prescription in cardiovascular rehabilitation: bridging the gap between best evidence and clinical practice. Front Cardiovasc Med. 2024;11:1380639.
28. Raisi A, Boonpor J, Breheny M, et al. Association of stair use with risk of major chronic diseases. Am J Prev Med. 2024;66:324-32.
29. Sanchez-Lastra MA, Ding D, Dalene KE, Del Pozo Cruz B, Ekelund U, Tarp J. Stair climbing and mortality: a prospective cohort study from the UK Biobank. J Cachexia Sarcopenia Muscle. 2021;12:298-307.
30. Song Z, Wan L, Wang W, et al. Daily stair climbing, disease susceptibility, and risk of atherosclerotic cardiovascular disease: a prospective cohort study. Atherosclerosis. 2023;386:117300.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0











Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.