


Pharmacologic management of metabolic and alcohol-associated liver disease
 0
0 Abstract
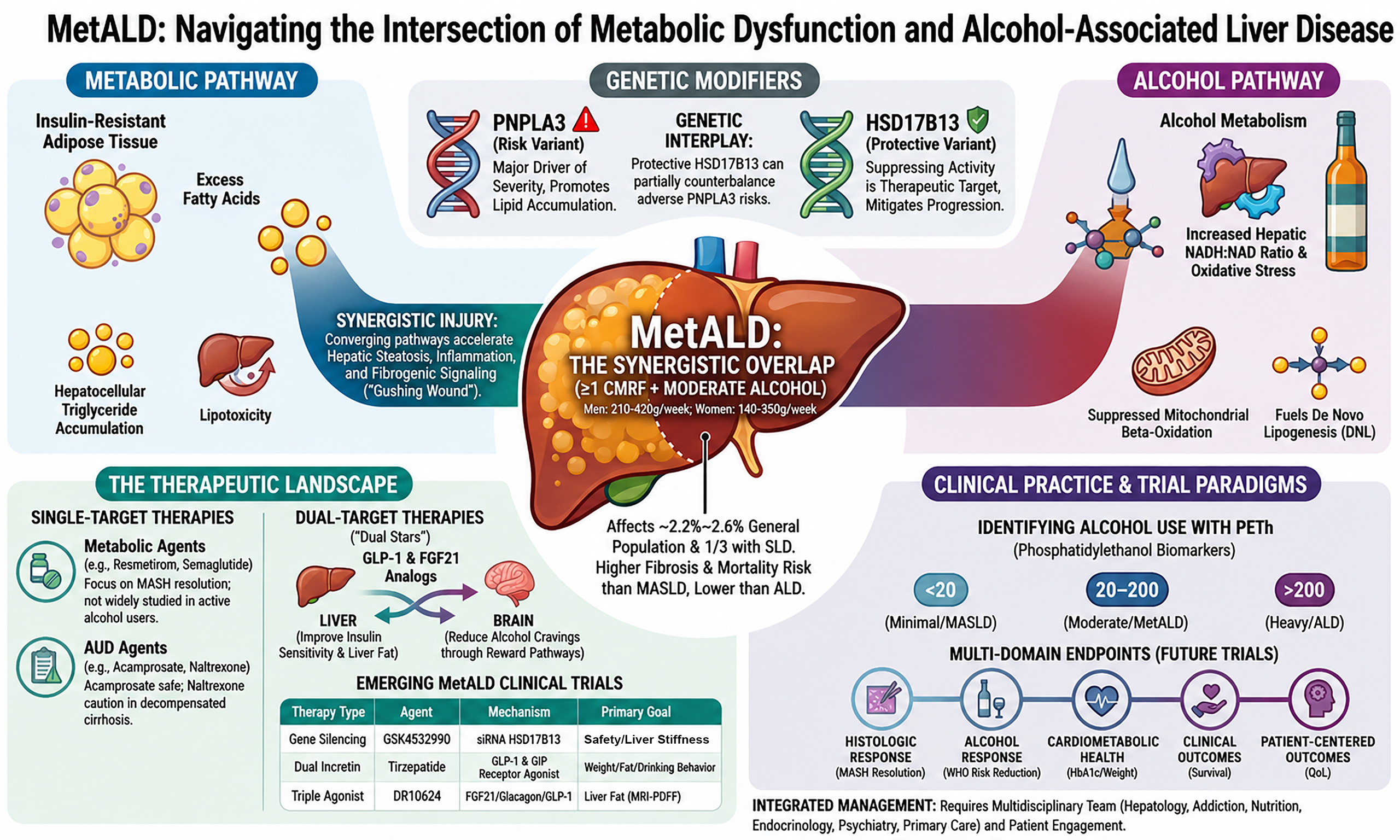
Metabolic dysfunction and Alcohol associated Liver Disease (MetALD) is an emerging phenotype within the steatotic liver disease spectrum, characterized by cardiometabolic risk factors coexisting with alcohol exposure, resulting in synergistic liver injury and fibrosis progression. Therapeutic development remains limited because most steatotic liver disease trials exclude patients with ongoing alcohol use. In contrast, alcohol-associated liver disease (ALD) trials have focused primarily on severe alcohol-associated hepatitis. Current management of patients with MetALD relies on an integrated approach that simultaneously controls alcohol use and cardiometabolic risk. In clinical practice, for patients with MetALD and ongoing alcohol use, therapies aimed at controlling alcohol use remain most critical, given the faster, more progressive disease course related to alcohol as compared to metabolic liver injury. Given the dynamic nature of alcohol intake and metabolic risk factors, longitudinal monitoring of disease stage with noninvasive fibrosis tests is essential. Liver-directed therapies with efficacy in metabolic dysfunction-associated steatotic liver disease (MASLD), including incretin-based agents, fibroblast growth factor 21 analogs, peroxisome proliferator-activated receptor agonists, and thyroid hormone receptor beta agonists, may benefit selected MetALD patients. Several agents may modulate both metabolic pathways and alcohol consumption through central reward mechanisms. Specific pharmacotherapies targeting alcohol use (acamprosate, naltrexone) combined with structured psychosocial interventions are effective in controlling alcohol use. Given the lack of dedicated clinical trials in MetALD patients, we synthesized data from clinical trials in MASLD and ALD. We propose adapting these data to inform the design of future clinical trials in patients with MetALD.
Keywords
INTRODUCTION
Metabolic dysfunction and Alcohol associated Liver Disease (MetALD) is a distinct subset of steatotic liver disease (SLD)[1]. MetALD is diagnosed in the presence of ≥ 1 cardiometabolic risk factor (CMRF) and 210-420 g/week of pure ethanol for men and 140-350 g/week for women[1,2]. CMRF in the context of SLD includes obesity or increased waist circumference, hypertension, type 2 diabetes mellitus, low high-density lipoprotein, and elevated triglycerides. The prevalence of MetALD from cohort studies is estimated at 2.2%-2.6% in the general population[3,4] and 31.8%-33.2% of individuals with SLD[5,6].
MetALD results from the synergistic interaction between metabolic dysfunction and alcohol. The two etiologies share underlying mechanisms, including dysregulated lipid and bile acid metabolism. As this is a new entity introduced under the SLD nomenclature, emerging data on the natural history indicate that individuals with MetALD have an intermediate risk of liver fibrosis, decompensation, and mortality, higher than metabolic dysfunction-associated steatotic liver disease (MASLD) but lower than alcohol-associated liver disease (ALD)[7]. Data are also emerging on the accuracy and cut-off points of serum and imaging-based non-invasive tests for assessing fibrosis in patients with MetALD.
In this narrative review, we will focus on the management of patients with MetALD. Simply utilizing treatments for MASLD and ALD independently, rather than within an integrated framework, would be a band-aid solution for a gushing wound. Hence, both risk factors need to be managed simultaneously with lifestyle modification and pharmacological therapies. Given the accelerated risk of progression with alcohol use compared to metabolic risk factors, the priority should be controlling alcohol use. Potential inaccuracy in self-reported alcohol use should be recognized, which underscores the role of biomarkers of alcohol intake to substantiate the information. Further, given the dynamic nature of the risk factors, especially alcohol use, periodic assessment of risk factors and the stage of liver disease should be performed[8].
A literature search was conducted in PubMed and ClinicalTrials.gov databases to identify studies related to MetALD, SLD, MASLD, metabolic dysfunction-associated steatohepatitis (MASH), ALD, alcohol use disorder, glucagon-like peptide 1 (GLP-1) receptor agonists, fibroblast growth factor 21 (FGF21) analogs, and thyroid hormone receptor-beta (THR-β) agonists. The search and manuscript preparation were completed, while the literature review included relevant preclinical studies, clinical trials, observational studies, practice guidelines, and review articles published between January 2010 and March 2026. Reference lists of selected articles were also manually screened to identify additional relevant studies. Articles were selected based on relevance to the pathophysiology, diagnosis, pharmacologic management, and clinical outcomes of MetALD and related SLD. Non-English articles, duplicate publications, and studies not directly relevant to MetALD, MASLD, ALD, or alcohol use disorder therapeutics were excluded.
THERAPEUTIC LANDSCAPE AND STRATEGIES TO MANAGE MetALD
Pathophysiologic rationale
Alcohol metabolism increases the hepatic NADH/NAD ratio, promotes oxidative stress, which in turn suppresses mitochondrial beta-oxidation, and enhances de novo lipogenesis (DNL)[2,9]. In parallel, insulin-resistant adipose tissue increases lipolysis and releases excess non-esterified fatty acids into the portal circulation, contributing to hepatocellular triglyceride accumulation, lipotoxicity, and downstream endoplasmic reticulum and mitochondrial stress[10]. The synergistic effects of the two risk factors augment hepatic steatosis, inflammation, and fibrogenic signaling in MetALD. Several observational studies have shown that individuals with MetALD have a higher prevalence of steatohepatitis, more advanced fibrosis, and an increased risk of hepatic decompensation compared with those exposed to either metabolic risk factors or alcohol alone[2,11]. Together, these data support a therapeutic framework for MetALD that targets the metabolic and inflammatory mechanisms driving liver injury, while alcohol use disorder is addressed in parallel through addiction-focused interventions.
Mechanistic plausibility, while necessary, is not sufficient to establish clinical efficacy. As in other areas of medicine, translation from bench to bedside in hepatology is associated with a high failure rate, as most phase 2 and 3 trials prioritize clinical outcomes over direct interrogation of underlying mechanisms. This limitation applies to all therapeutic targets discussed below.
MANAGEMENT OF CARDIO-METABOLIC RISK FACTORS
Non-pharmacologic management
Lifestyle modifications are a major part of treating MetALD. A weight-loss goal of ≥ 7%-10% is recommended to achieve beneficial effects on steatosis and fibrosis[12]. In the absence of weight loss, hepatic and cardiometabolic benefits can also be achieved by improving diet quality and physical activity[13]. Lifestyle interventions should adopt an approach that addresses diet, exercise, smoking, alcohol intake, and sleep. Mediterranean-style diets rich in unsaturated fats and fiber are recommended[14,15]. Structured moderate-to-vigorous aerobic exercise for 150-240 min per week combined with resistance training reduces steatosis and preserves lean body mass[5]. For individuals who do not achieve meaningful weight loss with lifestyle and pharmacologic therapy, bariatric surgery may be considered[16]. In a meta-analysis, bariatric therapies in MASH showed a 72% reduction in intrahepatic fat at 6 months and a 50% reduction in NAFLD activity score (NAS) at 36-60 months[17]. CMRF should be controlled by optimizing blood pressure, blood sugar, lipids, and smoking cessation[15]. High-intensity statins are the primary therapy for dyslipidemia, are safe, and should be used whenever indicated[18].
Pharmacologic management
The drug development landscape for SLD in MASLD patients is extensive [Table 1]. This has led to Food Drug Administration (FDA) approval of resmetirom, a THR-β agonist, in March 2024, and semaglutide, a GLP-1 receptor agonist, in August 2025, for the treatment of MASH patients with fibrosis stages 2-3[19,20]. However, these drugs were not studied in patients with MetALD. On the other hand, the drug development landscape in ALD has been relatively less advanced and has focused mainly on the severe form of alcohol-associated hepatitis (AH). Clearly, there is an unmet clinical need to assess the safety and efficacy of available drugs and to develop new targets for the population with MetALD. Further, divergent nutritional phenotypes in MetALD patients with obesity and CMRF on one side and malnutrition with nutrient deficiencies from alcohol use on the other (obese sarcopenia) are a challenge[21]. Drawing on the drug development landscape, we review therapeutic targets for patients with MetALD.
Ongoing clinical trials in MASH with potential relevance to MetALD*
| Drug class | Investigational agent | NCT number | Phase | Cirrhosis (F4) | Primary endpoint(s) |
| Incretin (GLP-1)** | Survodutide | NCT06632457 | Phase 3 | Yes | Time to first occurrence of any component of the composite clinical endpoint (all-cause mortality, liver transplant, hepatic decompensation events, worsening MELD to ≥ 15, or progression to CSPH) |
| Incretin (GLP-1)** | Survodutide | NCT06632444 | Phase 3 | No | Resolution of MASH without worsening of liver fibrosis; ≥ 1-point improvement in fibrosis stage without worsening of MASH (Week 52) Time to first occurrence of any component of the composite clinical endpoint (all-cause mortality, liver transplant, hepatic decompensation events, worsening MELD to ≥ 15, or progression to CSPH) |
| Incretin** (GIP/GLP-1) | Tirzepatide retatrutide | NCT07165028 | Phase 3 | No | Time to first occurrence of any component of the composite endpoint for MALO |
| FGF21** | Efruxifermin | NCT06161571 | Phase 3 | No | Incidence of adverse events and safety outcomes over 52 weeks. Changes in clinical and laboratory parameters over week 52 |
| FGF21** | Efruxifermin | NCT06528314 | Phase 3 | Yes | Time from randomization to first occurrence of disease progression as measured by a composite of protocol-specified clinical events in 5 years Cohort 1 only: ≥ 1-stage improvement in fibrosis with no worsening of steatohepatitis at 96 weeks |
| FGF21** | Pegozafermin | NCT06419374 | Phase 3 | Yes | Time to first occurrence of disease progression based on composite clinical events; fibrosis regression by ≥ 1 stage at Month 24 Time to occurrence of disease progression upto 5 years |
| FGF21** | Pegozafermin | NCT06318169 | Phase 3 | No | Co-primary endpoints at Week 52: fibrosis improvement by ≥ 1 stage without worsening of MASH; MASH resolution without worsening of fibrosis |
| PPAR agonist | Lanifibranor | NCT04849728 | Phase 3 | No | MASH resolution without worsening of fibrosis; fibrosis improvement by ≥ 1 stage without worsening of MASH week 72 |
| THR-β | Resmetirom (MAESTRO- NASH OUTCOMES) | NCT05500222 | Phase 3 (ongoing) | Yes | Incidence of adjudicated composite clinical outcome event (all-cause mortality, liver transplant, ascites, hepatic encephalopathy, gastroesophageal variceal hemorrhage, or MELD increase from < 12 to ≥ 15 due to liver disease) |
| SGLT2 | Empagliflozin | NCT06117137 | Phase 3 | No | Number of participants with treatment-related adverse events (CTCAE v4.0); number of participants with tightly controlled diabetes mellitus (6 months) |
| Incretin** (GCG/GLP-1) | Efinopegdutide | NCT04505436 | Phase 2 | No | Resolution of MASH with no worsening of fibrosis |
| Incretin** (GCG/GLP-1) | Efinopegdutide | NCT06465186 | Phase 2 | Yes | Change from baseline in LFC at Week 28; Adverse events up to week 36 and discontinuation rates up to week 28 |
| Incretin** (GCG/GLP-1) | AZD9550 AZD6234 | NCT06151964 | Phase 2 | No | Number and percentage of participants with any adverse event, serious adverse events, or adverse events leading to discontinuation upto day 205 |
| FGFR and VEGFR inhibitors | BI 3802876 | NCT07325526 | Phase 2 | Yes | Occurrence of any AEs up to 134 days |
| THR-β agonist | HSK31679 | NCT06168383 | Phase 2 | No | Proportion of patients with MASH resolution (2-point reduction in NAS with at least 1-point reduction in ballooning and no increase in steatosis) and no worsening of fibrosis at Week 52 |
| THR-β agonist | ASC 41 | NCT05462353 | Phase 2 | No | Reduction in liver fat content, typically measured via MRI-PDFF, alongside safety and tolerability assessments |
| Genetic (RNAi) | ALN-HSD- HSD17B13-RNAi | NCT05519475 | Phase 2 | No | Change in the continuous qFibrosis score measured by second harmonic generation/two-photon excitation microscopy up to week 52 |
| HSD17B13** | GSK4532990 | NCT05583344 | Phase 2 | Both F3-F4 | Percentage of participants achieving ≥ 1-stage improvement in histologic fibrosis with no worsening of NASH; percentage achieving NASH resolution with no worsening of fibrosis (F3 cohort, Week 52) |
| ACE inhibitor | Lisinopril | NCT04550481 | Phase 2 | No | Change in PRO-C3 values week 24 |
| PDE inhibitor | ZSP1601 | NCT05692492 | Phase 2 | No | Resolution of MASH with no worsening of fibrosis; fibrosis regression by ≥ 1 stage |
| Fibrate | Pemafibrate | NCT06623539 | Phase 2 | No | Change in ALT week 24 |
| PNPLA3 | LY3849891 | NCT05395481 | Phase 1 | No | Number and percentage of participants with any adverse event week 26 Mean change from baseline on liver inflammation and fibrosis content measured by MRI at 24 weeks |
| Anti-TL1A antibody | Afimkibart, (RO7790121) | NCT06903065 | Phase 1 | Yes | Percentage of participants with AEs up to Week 52 |
Drugs modulating insulin resistance
Incretin based therapies (GLP-1 receptor agonists and dual GLP1/GIP agonists)
The clinical trials on GLP-1 receptor agonists have been mainly performed in patients with MASLD and MASH, and excluded patients with excess alcohol use [Table 1]. Incretin-based agonists to receptors, including GLP-1 (exenatide, liraglutide, and semaglutide), dual GLP-1/gastric inhibitory polypeptide or GIP (tirzepatide), or GLP-1 and glucagon receptor (survodutide), and triple agonists (retatrutide), have gained increasing attention[22]. These agents promote weight loss, improve insulin sensitivity, and reduce systemic and hepatic inflammation. In addition, emerging data suggest a role in modulating alcohol intake through central appetite and reward pathways[23,24]. GLP-1 receptor agonists exert central and peripheral effects through the gut-brain axis, promoting satiety, delaying gastric emptying, and reducing caloric intake, and improve mitochondrial function by suppressing DNL[25].
In a phase 2 randomized trial of 190 patients with biopsy-proven MASH, once-daily semaglutide administered for 52 weeks resulted in significantly higher rates of MASH resolution without worsening fibrosis compared with placebo[26]. More recently, results from the phase 3 ESSENCE trial demonstrated that 72 weeks of semaglutide therapy led to MASH improvement in 62.9% of treated patients, compared with 34.1% with placebo, and fibrosis improvement in 37%, compared with 22.5% with placebo (P < 0.0001 for both endpoints)[27]. Dual incretin therapy with tirzepatide has also demonstrated a reduction in hepatic steatosis, as measured by imaging-based liver fat quantification at one year, though histologic outcomes remain under investigation[28].
FGF21 analogs
FGF21 is a hormone with endocrine, autocrine, and paracrine activity. It is produced predominantly by the liver, adipose tissue, and other organs[29,30]. FGF21 exerts its metabolic effects primarily by promoting lipid catabolism and increasing insulin sensitivity, thereby enhancing lipolysis, fatty acid mitochondrial beta-oxidation, and energy dissipation. It also modulates appetite via a central mechanism and decreases preference for sugar and alcohol. Collectively, these effects reduce hepatic lipotoxicity, inflammation, and fibrogenesis, supporting its role in SLD and steatohepatitis[31,32].
In phase 2 studies, the FGF21 analog efruxifermin reduced the hepatic fat fraction. Among patients with MASH cirrhosis, 25% achieved MASH resolution, including at least one stage of fibrosis improvement[33]. In a recent meta-analysis of eight randomized trials involving 963 MASH patients, FGF21 analogs (efruxifermin, pegbelfermin, and pegozafermin) were superior to placebo in improving liver fibrosis by ≥ 1 stage (27% vs. 14%), with a pooled risk ratio of 1.83 (1.27-2.62). FGF21 showed class heterogeneity. For example, a subgroup analysis on at least two-point reduction in NAS without worsening of fibrosis showed the lowest efficacy with pegozafermin (RR = 2.48; 95%CI: 1.57-3.93; P = 0.0001) and the highest with efruxifermin (RR = 3.50; 95%CI: 2.01-6.08; P < 0.00001)[34].
Peroxisome proliferator-activated receptor agonists
Peroxisome proliferator-activated receptor (PPAR) agonists target lipid metabolism, insulin sensitivity, inflammation, and fibrogenesis[35], to enhance hepatic fatty acid oxidation. Specifically, PPAR β and δ receptors promote thermogenesis and reduce lipogenesis, while PPAR γ improves insulin sensitivity. These beneficial effects modulate inflammatory and fibrotic signaling[36,37].
Lanifibranor, a pan-PPAR agonist, in a phase 2b trial (NATIVE trial) among MASH patients, showed a ≥ 2-point reduction in the NAS in 55% of patients receiving lanifibranor vs. 33% of patients receiving placebo. In treated patients, NASH resolved in 49% and fibrosis improved by at least 1 stage in 48%.
Saroglitazar, a dual PPAR α γ agonist, improved steatosis and fibrosis and additionally led to decreased cardiovascular risk in MASH[38,39]. Pioglitazone, a selective PPARγ agonist, has also demonstrated improvements in steatosis and inflammation, with benefits for fibrosis and MASH resolution.
Sodium glucose co-transporter -2 inhibitors
Sodium glucose co-transporter -2 (SGLT2) inhibitors improve glucose control and may promote weight loss. In clinical trials, Ipragliflozin, compared to placebo, improved liver outcomes in diabetic patients with MASH, including fibrosis[40]. In a meta-analysis of randomized controlled trials in MASH patients, SGLT2 inhibitors were associated with improvements in steatosis and liver fibrosis[41].
Drugs targeting de-novo-lipogenesis
THR-β agonists
THR-β is a nuclear receptor involved in hepatic fatty acid β-oxidation, mitochondrial biogenesis, and cholesterol clearance. Because THR-β is predominantly expressed in the liver, agonism of THR-β improves hepatic metabolism without the extrahepatic effects of THR-α[42].
In the MAESTRO NASH trial in patients with biopsy-proven NASH with F1b to F3 fibrosis, resmetirom 80 and 100 mg at 52 weeks achieved resolution of NASH without worsening of fibrosis in 25.9% and 29.9%, respectively, compared with 9.7% in the placebo group. Improvement in fibrosis by at least one stage was observed in 24.2% and 25.9% of patients receiving 80 and 100 mg, respectively, compared with 14.2% of patients receiving placebo. Furthermore, there was a significant reduction in low-density lipoprotein cholesterol in the resmetirom arms but not in the placebo arm.
FXR agonists
These agonists target bile acid-mediated signaling pathways that regulate lipid and glucose metabolism, insulin sensitivity, and downstream metabolic and inflammatory pathways[43].
Several non-bile acid Farnesoid X receptor (FXR) agonists have shown encouraging results in early-phase studies. For example, cilofexor improved hepatic fibrosis without worsening steatohepatitis when combined with the acetyl-CoA carboxylase (ACC) inhibitor firsocostat in a phase 2 study[44]. Tropifexor demonstrated dose-dependent reductions in liver enzymes and hepatic fat fraction in a randomized phase 2 trial in patients with MASH[45]. Vonafexor, evaluated in the LIVIFY phase 2a trial, was generally well tolerated and associated with significant reductions in liver fat, liver enzymes, and body weight as assessed by magnetic resonance imaging and biochemical markers[46].
Inhibitors of DNL and triglyceride synthesis
Key enzymatic targets of DNL include fatty acid synthase (FAS), ACC, ATP citrate lyase, and diacylglycerol acyltransferase (DGAT), which together regulate fatty acid synthesis and triglyceride formation in hepatocytes[47].
Denifanstat, an oral FAS inhibitor, demonstrated histologic efficacy in the phase 2b FASCINATE 2 trials in patients with F2-3 MASH[48]. At 52 weeks, patients treated with denifanstat, compared with placebo, achieved a two-point or greater reduction in NAS without worsening of fibrosis in 38 percent vs. 16 percent; resolution of MASH in 26 percent vs. 11 percent; fibrosis regression of at least one stage in 49 percent vs. 13 percent; and reduction in liver fat on magnetic resonance imaging proton density fat fraction (MRI-PDFF) in 31 percent vs. 10 percent. In addition, denifanstat rapidly lowered tripalmitin, a biomarker of DNL. DGAT2 inhibitors, such as ervogastat, have demonstrated reductions in liver fat in short phase 2 studies, either as monotherapy or in combination regimens[49].
Genetic modifiers of hepatic lipid accumulation and treatment response
The Patatin-Like Phospholipase Domain Containing 3 (PNPLA3) and HSD17B13 genetic polymorphisms are most commonly established in the development and severity of SLD, including MetALD[50]. The PNPLA3 I148M variant is associated with increased steatosis, progression of fibrosis, and greater severity of SLD, including MetALD. In contrast, HSD17B13 loss- of-function variants appear protective against progressive liver injury. When both variants are present, the protective effect of HSD17B13 may partially attenuate the adverse risk associated with PNPLA3[51,52]. The therapeutic targeting of HSD17B13 is currently being evaluated in a Phase 2 clinical trial (NCT06613698) in patients with MetALD.
Currently, several promising agents are advancing through clinical development and have the potential to be approved treatment options for MASH. These include FGF21 analogs such as efruxifermin and pegozafermin[33], PPAR agonist lanifibranor[53], and Survodutide[54]. Of these, resmetirom and efruxifermin are also being evaluated in patients with MASH cirrhosis (F4). These trials are designed to assess the safety and efficacy of the intervention as a pathway to regulatory drug approval, and they vary across countries depending on the respective regulatory frameworks, alcohol use patterns, disease prevalence, and healthcare access.
Combination therapeutic approaches
Given multiple therapeutic targets with distinct mechanisms, combination therapy represents a promising strategy to enhance therapeutic efficacy. Several clinical trials are currently underway that use combinations of different agents [Table 2]. Of particular interest are combinations of GLP-1 receptor agonists with FGF21 analogs (NCT05016882), the SGLT2 inhibitor empagliflozin with PPAR agonists (NCT04976283), and with GLP-1 receptor agonists (NCT04639414).
Combination pharmacotherapy trials in MASH: key drug classes, regimens, and clinical trial phases
| Drug class/Combination | Investigational agents | NCT number | Study phase |
| SGLT2 + PPAR ± Metformin | Empagliflozin + Pioglitazone + Metformin | NCT04976283 | Phase 4/real world |
| SGLT2 + GLP-1 | Empagliflozin + Semaglutide | NCT04639414 | Phase 4/real world |
| Incretins comparators | Tirzepatide vs. Retatrutide (Master protocol) | NCT07165028 | Phase 3 |
| FGF21 + GLP-1 | Zalfermin (NNC0194-0499) + Semaglutide | NCT05016882 | Phase 2 |
| PPAR + SGLT2 | Lanifibranor + Empagliflozin | NCT05232071 | Phase 2 |
| GLP-1 + FXR + ACC | Semaglutide + Cilofexor + Firsocostat | NCT04971785 | Phase 2 |
| ASK1 + FXR + ACC | Selonsertib + Cilofexor + Firsocostat | NCT03449446 | Phase 2 |
Gut-liver axis targeted therapies
Despite recognition of the role of gut dysbiosis in MASLD, clinical translation remains limited. In a randomized controlled trial, fecal microbiota transplantation (FMT) in MASLD patients showed a trend toward lower serum triglyceride levels but no change in hepatic fat content or metabolic parameters at 12 weeks[55].
Overall, the emerging therapeutic landscape for MetALD suggests that no single agent is likely to address the full spectrum of underlying processes in this population. Incretin-based therapies currently have the most established clinical evidence and may offer benefits for both metabolic dysfunction and alcohol-related behaviors. FGF21 analogs are also of particular interest for their potential dual metabolic and alcohol-modulating effects. However, dedicated studies in MetALD are lacking for both GLP-1 and FGF21 agonists. THR-β agonists such as resmetirom appear promising for fibrosis-directed therapy, while PPAR agonists may have a role in carefully selected patients. Given the heterogeneity and dynamic nature of MetALD, future management will likely require individualized, potentially combination-based approaches targeting both metabolic dysfunction and alcohol use.
THERAPIES FOR ALCOHOL USE DISORDER
Non-pharmacologic management
Abstinence improves long-term outcomes in patients with liver disease and comorbid alcohol use disorder (AUD)[56]. Evidence-based nonpharmacological treatments for AUD include motivational interviewing with brief intervention to counsel patients on alcohol-related harms, cognitive-behavioral therapy, motivational enhancement therapy, contingency management approaches, couples and family counseling, and 12-step facilitation therapy[57]. Psychosocial interventions are more effective when combined with pharmacological therapies[58].
Pharmacological therapies
FDA-approved medications for alcohol use disorder (MAUD) include disulfiram, naltrexone, and acamprosate[59-61]. Nalmefene is approved by the European Medicines Agency but is not available in the US for the treatment of AUD[59,62]. [Table 3].
Investigational agents in MetALD: active trials and mechanistic targets
| NCT number | Phase | Drug | Mechanism tested | Completion | Primary endpoint(s) |
| NCT06613698 | 2 | GSK4532990 | siRNA targeting HSD17B13 to reduce expression of a hepatocyte droplet protein linked to alcohol related and metabolic liver injury | Mar 30, 2028 | Number of participants with AEs/SAEs (up to 8 weeks) Clinically relevant ECG/vital sign/laboratory changes (up to 8 weeks) Change from baseline in liver stiffness by FibroScan at week 28; change from baseline in MELD score at week 28 |
| NCT07046819 | 2 | Tirzepatide | Dual GLP-1/GIP receptor agonist aimed at reducing body weight, liver steatosis, and possibly alcohol related behaviors in MetALD | Jul 30, 2026 | Metabolic improvement from baseline measured by percentage reduction in body weight Reduction in liver steatosis measured by FibroScan CAP score |
| NCT07024212 | 2 | DR10624 injection | Long-acting tri-agonist targeting FGF21R, GLP-1R, and GCGR to improve steatosis, insulin sensitivity and weight regulation | Jun 30, 2026 | Relative percentage changes (%) of LFC from baseline to Week 12, assessed by MRI-PDFF |
Acamprosate is not metabolized in the liver and is safe in patients across the spectrum of ALD. However, randomized trials in patients with ALD are lacking. In a small, open-label phase II trial of 12 patients with ALD, acamprosate reduced craving scores in all participants with no adverse events[63]. A dose reduction is necessary in patients with renal impairment. Baclofen, gabapentin, and topiramate are additional options for patients unable to take acamprosate or naltrexone, as they are not significantly metabolized in the liver, though they require renal dose adjustment.
Dual targets
Incretin-based therapies
Observational data suggest that incretin-based therapies may reduce alcohol intake in some individuals with obesity and AUD[64,65]. In a retrospective analysis of 153 obese individuals, 106 patients treated with GLP-1-based therapies (semaglutide and tirzepatide) reported a reduction in alcohol intake after treatment initiation, compared with 47 control patients not receiving incretin therapy[66]. Similar observational findings have been reported in other retrospective cohorts, suggesting a potential class effect[64,67]. These observational studies relied on propensity score matching to account for differences between treatment groups and did not account for unmeasured confounding, reverse causation, healthy-user bias, or publication bias. These limitations constrain causal interpretation of these observations.
Clinical trials that achieve comparability by allocating treatment groups randomly across participants are needed to corroborate these encouraging observational findings.
Randomized controlled trials are limited by sample size, varying interventions and durations, and inconsistent results: two studies showed benefit, while one showed no benefit[23]. However, none of these three trials recruited patients with liver disease.
FGF21 analogs
FGF21 is uniquely positioned as alcohol increases endogenous circulating FGF21 levels. FGF21 signaling may additionally reduce alcohol consumption through central reward pathways[68-70]. Furthermore, human genetic analyses using Mendelian randomization provide strong causal evidence that enhanced FGF21 signaling reduces alcohol consumption and the risk of alcohol use disorder[71]. Although there is strong experimental data, clinical trials are needed to examine the benefit of FGF21 agonists in reducing alcohol intake in patients with ongoing alcohol use.
THR-β agonists
THR-β agonists reduced steatosis and liver injury in preclinical ALD models, but clinical data in patients with alcohol use remains lacking[72].
PPAR agonists
Preclinical studies suggest PPAR agonists may influence alcohol intake[73,74]. The only available human study using pioglitazone in 16 subjects reported increased alcohol craving and risk of myopathy, leading to early termination of the study[75]. In contrast, the PPARα agonist fenofibrate has shown reduced voluntary alcohol consumption in rodent models[76-78]. Mechanistic studies suggest modulation of GABAergic interneurons within the amygdala[74]. Taken together, signals of increased alcohol craving with pioglitazone and the limited human data on dual agonists in active alcohol use indicate that well-designed studies in carefully selected patients are needed to substantiate the role of these drugs for alcohol use.
Inhibitors of DNL and triglyceride synthesis
In the absence of clear effects on alcohol related metabolic pathways, these agents may have a limited role in patients with active alcohol use and may be better suited for individuals with MetALD who have achieved sustained reduction or remission of alcohol intake, pending dedicated clinical studies.
Drugs targeting gut-liver-brain axis
Chronic alcohol use impairs the intestinal barrier and alters gut microbiota composition[79]. Bacterial products penetrate the impaired intestinal barrier, triggering hepatic and systemic inflammation and microbiome changes that disrupt the enterohepatic circulation of bile acids[80]. In a randomized placebo-controlled trial involving 46 patients with moderate AH, Lactobacillus rhamnosus GG supplementation (n = 22) compared to placebo resulted in significant improvements in model for end-stage liver disease (MELD) score at 1 month and reduced alcohol consumption at 6 months[81]. In a randomized phase 1 trial on 20 patients with ALD cirrhosis and AUD, FMT enema (n = 10) compared to placebo reduced alcohol craving and consumption, with favorable microbial changes[82]. Although promising, these two high-quality trials of interventions to restore gut dysbiosis remain proof-of-concept. Further, none of these trials included patients with MetALD. Clearly, future trials with larger sample sizes in the MetALD population are needed before these results can inform clinical practice.
Gene editing therapy for AUD
Gene-editing therapies, such as clustered regularly interspaced short palindromic repeats (CRISPRs), may be used to modify genes encoding alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH), enzymes involved in alcohol metabolism[80,83].
Current landscape of clinical trials in MetALD
The therapeutic landscape for MetALD is evolving from treating MASH and ALD separately to integrated management targeting both risk factors [Figure 1][84,85]. Management of MetALD focuses on alcohol cessation and optimization of CMRF. However, several features warrant consideration when designing clinical trials in MetALD. Given the unique nature of this condition, accurate information on alcohol use, complemented by phosphotidylethanol (PEth) testing, will be required to define the population. Further, we need to recognize that alcohol use limits to identify MetALD are based on consensus and have not been validated across populations with divergent patterns of alcohol use. Understanding how variations in drinking patterns across cultures and countries may produce different pathophysiologic consequences and require different therapeutic strategies. Beyond overall safety assessment, these trials would need to examine the interaction of the drug with other medications used for managing metabolic comorbidities and with ongoing alcohol use. For example, resmetirom interacts with statins and clopidogrel when prescribed simultaneously to patients with MASLD and MetALD. Hence, it is recommended to limit the statin dose to a maximum of 20 mg (simvastatin and rosuvastatin) and 40 mg (pravastatin and atorvastatin), and to reduce the resmetirom dose by 20 mg in patients taking clopidogrel. As gemfibrozil is a strong inhibitor of the Cytochrome P (CYP) pathway involved in resmetirom metabolism, it is contraindicated for the treatment of dyslipidemia in patients taking resmetirom. Similar interactions are not known for semaglutide or acamprosate. Studies would also need to assess sarcopenia and its interaction with drug efficacy and pharmacokinetics. The optimal cut-off for non-invasive tests for fibrosis assessment to select the patient population and identify clinically meaningful changes at follow-up would need to be determined to inform pathways for drug approval in patients with MetALD.
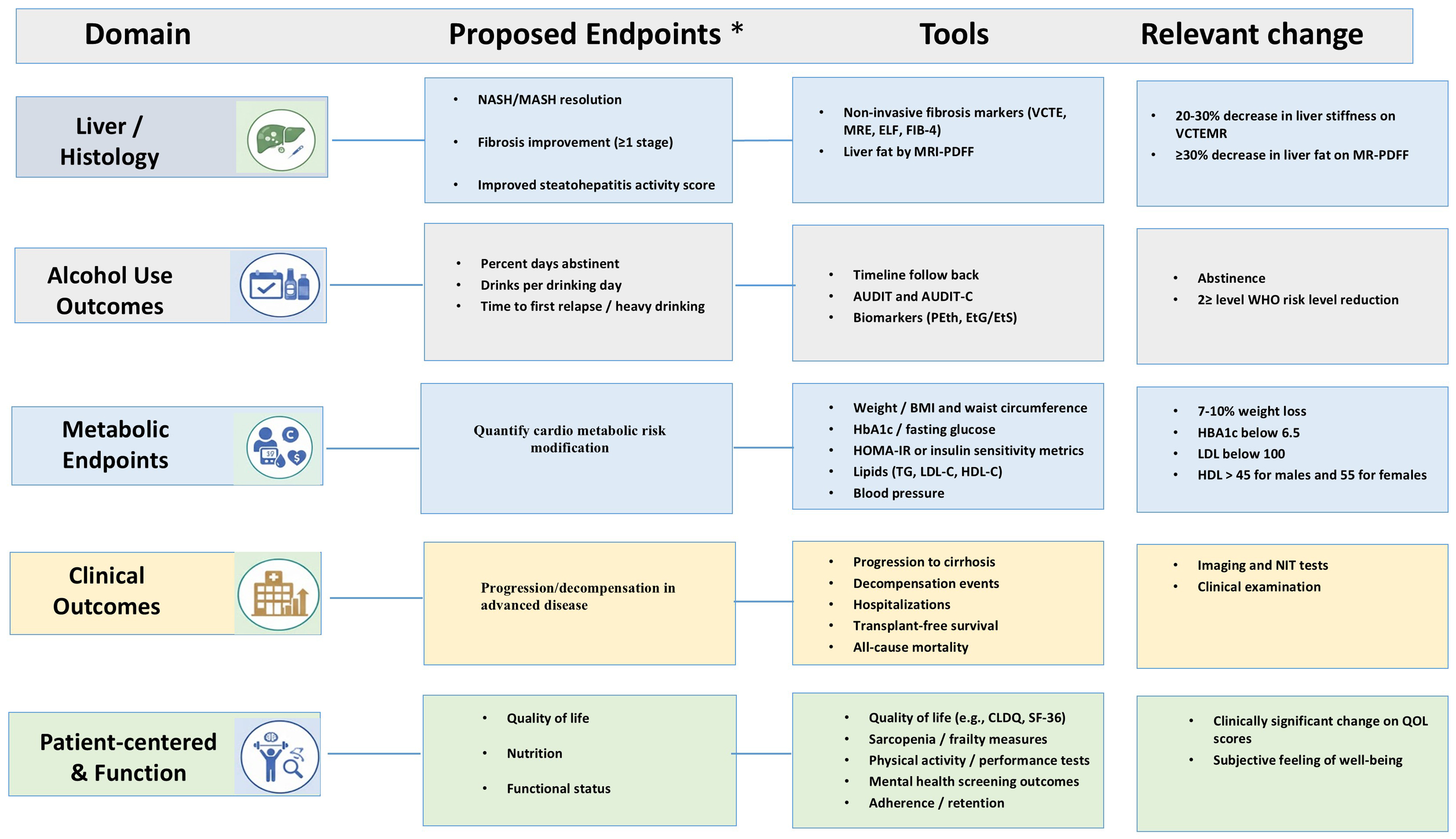
Figure 1. Proposed Endpoint Domains and Measures for MetALD Clinical Trials. *Integrated efficacy monitoring algorithm (month 12 and annually). Histologic response: MASH resolution without worsening of fibrosis, and/or fibrosis improvement ≥ 1 stage without worsening of steatohepatitis. NIT: ≥ 30% reduction in MRI-PDFF; LSM ↓ ≈ 20% from baseline and/or improvement in biomarker NIT from baseline (ELF, FIB-4) from baseline. Alcohol-use response: Abstinence and ≥ 2 WHO risk level reduction on alcohol use (abstinence is no alcohol use; low level is 1-20 g/d for women and 1-30 g/d for men; moderate level is 21-40 g/d for women and 31-60 g/d for men; high level is 41-60 g/d for women and 61-100 for men; and very high level is > 60 g/d for women and >100 g/d for men). Cardio metabolic response: weight ↓ ≥ 5%-10% or waist ↓; HbA1c ↓ ≥ 0.5% or improved fasting glucose; HOMA-IR ↓; TG/LDL-C ↓, HDL-C ↑; BP ↓ or controlled. Clinical outcomes: no progression to cirrhosis; absence of decompensation (ascites, variceal bleeding, encephalopathy); reduced hospitalizations; improved transplant-free survival; reduced mortality. Patient-centered outcomes: QoL ↑ (CLDQ/SF-36); sarcopenia/frailty ↓; physical performance ↑; mental health scores ↑; adherence/retention ↑. ↑ Increase; ↓ decrease. BMI: Body mass index; CLDQ: Chronic Liver Disease Questionnaire; ELF: Enhanced Liver Fibrosis test; EtG: ethyl glucuronide; EtS: ethyl sulfate; FIB-4: Fibrosis-4 index; HbA1c: hemoglobin A1c; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: Homeostasis Model Assessment of Insulin Resistance; LDL-C: low-density lipoprotein cholesterol; MASH: metabolic dysfunction-associated steatohepatitis; MRE: magnetic resonance elastography; MRI-PDFF: magnetic resonance imaging-proton density fat fraction; NASH: nonalcoholic steatohepatitis; PACS: Penn Alcohol Craving Scale; PEth: phosphatidylethanol; SF-36: 36-Item Short Form Health Survey; TG: triglycerides; VCTE: vibration-controlled transient elastography.
An ideal pharmacological approach to treat MetALD patients would be ‘dual targets’, that are effective against SLD and reducing alcohol use. Of the potential targets discussed earlier, GLP-1 and FGF21 agonists are the best candidates for clinical trials in MetALD, as these agents have the strongest evidence of metabolic benefits and the potential to reduce alcohol use [Table 4]. Given the challenges of defining this population and its underrepresentation in clinical drug development, we suggest that ongoing trials in the MASLD and ALD space should measure ongoing alcohol use to perform subgroup analyses in MetALD patients, such as the MAESTRO NASH trial. In a subgroup of 75 patients meeting alcohol use and PEth criteria for MetALD, improvements in fibrosis and MASH were observed, similar to MASH patients[19,42]. These data, based on post-hoc analysis of the trial in a small sample of MetALD patients, do suggest a potential role for THR-β agonists, although dedicated trials to examine this hypothesis are needed before their use in practice for patients with MetALD. Taken together, resmetirom, incretin-based therapies, and FGF21 analogs represent promising therapeutic agents that have yet to be fully evaluated in clinical trials.
Alcohol-directed pharmacological therapies for MetALD
| Drugs | Therapeutic effect | Comments | |
| Medications for alcohol use disorder | |||
| FDA approved medications | Acomprosate 61-63, 65 | Reduces heavy drinking manages cravings during abstinence | NNT =11 to prevent return to any drinking Caution with renal disease |
| Disulfiram | Blocks breakdown of alcohol | Not recommended for use in liver disease | |
| Naltrexone 62, 64 (oral and Inj) | Reduces heavy drinking Manages cravings | NNT = 18 for oral naltrexone Interaction with opioids | |
| Non-FDA approved medications | Topiramate 61, 63 | 2nd line treatment | Caution in hepatic encephalopathy |
| Gabapentin 61-63 | 2nd line treatment | Caution in hepatic encephalopathy | |
| Varenicline 61-63 | Not studies in ALD | Emerging evidence to support its use | |
| Baclofen 61-63 | Not FDA approved | Can be used safely in ALD | |
| Nalmefene 61, 64 | Not FDA approved | Reduce alcohol consumption in combination with psychological support | |
| Dual targets | |||
| GLP-1 RA (Ozempic) 66, 67 | Improves metabolic dysfunction and reduces cravings | Phase 2 and phase 3 | |
| Fibroblast growth factor 21 (FGF21) analogues 72, 73 | Experimental, reduces alcohol intake in primates | Preclinical | |
| Experimental therapies | |||
| Fecal Microbiota Transplantation 85, 86 | Investigational | Phase 1 and phase 2 | |
| Gene editing therapy (TALENs and CRISPR/Cas9) 83, 86 | Under investigation | ||
CURRENT THERAPEUTIC APPROACH TO MANAGE METALD
MetALD liver injury creates a heterogeneous population in whom sustained abstinence is necessary but rarely sufficient. Therefore, to target both alcohol use and metabolic dysfunction, current management focuses on a combination of lifestyle modifications, management of CMRF, and pharmacotherapy [Table 5][86]. The interaction between two risk factors is sometimes counterintuitive in the management of patients with MetALD. For example, individuals undergoing bariatric surgery, especially Roux-en-Y gastric bypass surgery for weight loss, can trigger new-onset or worsen ongoing alcohol use[87].
Integrated management framework for MetALD: lifestyle, AUD treatment, and metabolic therapies
| Category | Key interventions | Outcomes |
| Lifestyle and behavioral | Mediterranean/energy-restricted diets; 150-240 min/week moderate-vigorous aerobic exercise; resistance training; bariatric/metabolic surgery when appropriate | ≥ 7%-10% weight loss is central; benefits even without weight loss; integrated 24-h lifestyle approach; bariatric surgery reduces intrahepatic fat and NAS and improves fibrosis |
| Manage cardio -metabolic risk | Aggressive management of diabetes, dyslipidemia, hypertension, obesity and OSA; statins; GLP-1 RAs and SGLT-2 inhibitors | Optimizing blood pressure, lipids and glycaemia reduces cardiovascular risk; statins safe across MASLD spectrum; screen and treat OSA; GLP-1 RAs/SGLT-2 inhibitors improve steatosis, weight and cardiovascular outcomes |
| AUD pharmacotherapy | Structured psychosocial interventions; acamprosate; naltrexone; consider baclofen, gabapentin, topiramate | Acamprosate increases abstinence and lacks hepatic metabolism; naltrexone reduces heavy drinking but avoid in Child-Pugh C; hepatic safety study showed decreased ALT/AST after naltrexone; baclofen and others provide alternatives |
| Metabolic pharmacotherapy | Resmetirom (THR-β agonist); GLP-1 RAs (semaglutide, liraglutide); SGLT-2 inhibitors | Resmetirom achieved NASH resolution in 25.9%-29.9% and improved fibrosis; GLP-1 RA trial showed 59% NASH resolution but no significant fibrosis improvement. GLP-1RA also improve weight, glycemic control and lipids |
| Microbiome and adjunctive | Faecal microbiota transplantation; probiotics; prebiotics | Consecutive FMT did not improve liver fat or metabolic parameters at 12 weeks; microbiome therapies remain experimental |
An algorithm for MetALD management involves targeting metabolic risk factors and alcohol [Figure 2]. The first step is to identify the current level of alcohol use using self-reported information (AUDIT-C or timeline follow-back tools), complemented with whole blood PEth level (ng/mL), a biomarker of alcohol metabolism with a window of detection of 3-4 weeks from last alcohol use[88]. A PEth level < 20 (minimal or no alcohol use) is consistent with MASLD, 20-200 (moderate alcohol use) is consistent with MetALD, and > 200 (heavy alcohol use) is consistent with ALD[89].
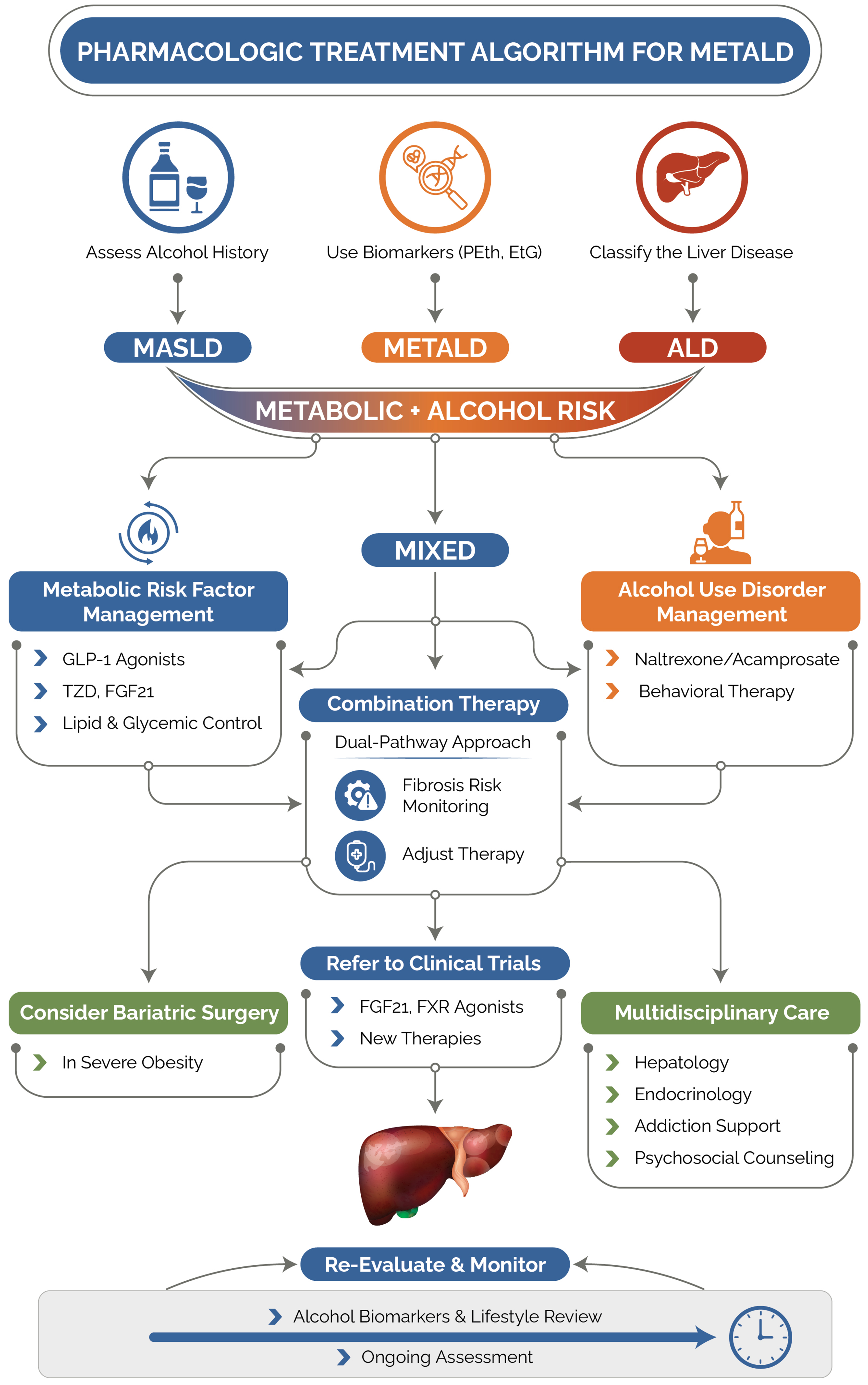
Figure 2. Proposed algorithm for management of patients with MetALD in clinical practice. ALD: Alcohol associated liver disease; EtG: ethyl glucuronide; FGF: fibroblast growth factor; GLP: glucagon-like peptide; MASLD: metabolic dysfunction-associated steatotic liver disease; MetALD: metabolic dysfunction and alcohol associated liver disease; PEth: phosphatidylethanol; T2DM: type 2 diabetes mellitus.
Controlling alcohol use is the most critical factor in patients with active ongoing use, as alcohol-induced injury is more progressive than metabolic liver injury. As the data on safe alcohol use in SLD patients remain unknown, the current recommendation is to abstain completely. For patients abstaining for 3-12 months (early recovery) or more than 12 months (stable recovery) who still have significant fibrosis (F2 or higher), the focus should be on liver-targeted treatments and control of metabolic comorbidities (https://www.niaaa.nih.gov/research/niaaa-recovery-from-alcohol-use-disorder/definitions) While awaiting safety data for drug therapy in MetALD cirrhosis patients, those with advanced fibrosis (F2-F3) should be considered for treatment with resmetirom or a GLP-1RA. Shared decision-making between the patient and the provider is critical, considering the route of administration and CMRF. For example, a patient with metabolic-predominant disease (diabetes mellitus, BMI > 35, and atherosclerotic disease) is better treated with a GLP-1 receptor agonist. Patients with MetALD who have F0-1 fibrosis stage or with cirrhosis do not currently have specific FDA-approved pharmacotherapies. A multidisciplinary, stepwise approach integrating hepatology, endocrinology, addiction medicine, nutrition, and mental health services is essential[16]. On follow-up, monitoring should include non-invasive tests for liver disease; alcohol use using the timeline follow-back tool and PEth test; metabolic comorbidities; nutritional assessment; and quality of life [Figure 2]. Continuing to re-evaluate patients for these outcomes can maximize the effectiveness of treatment for a changing phenotype with changes in alcohol use in MetALD.
SAFETY CONSIDERATIONS
A structured approach to safety reporting in MetALD should address patient selection, contraindications, monitoring, and risk stratification, given the overlap among liver injury, ongoing alcohol exposure, and metabolic comorbidity in this population. Risk stratification should identify patients who need closer surveillance during therapy, particularly those with ongoing alcohol use, advanced fibrosis, cardiometabolic disease, fluid retention, or baseline muscle loss, rather than relying on a single disease label.
PPAR agonists such as lanifibranor and saroglitazar may be less suitable for patients at risk of fluid retention or weight gain, given their association with approximately 8% to 10% rates of weight gain and edema[53]. For resmetirom, gastrointestinal (GI) adverse events are the most commonly reported, with similar rates of serious adverse events across treatment arms[19]. Cardiac safety in patients with liver disease and ongoing alcohol use remains insufficiently defined. A secondary analysis including 75 patients with “possible MetALD,” defined by elevated carbohydrate-deficient transferrin (CDT) > 2.5% or PEth > 20 ng/mL, demonstrated similar treatment responses at 52 weeks, regardless of alcohol use, suggesting potential efficacy and safety across the MASLD-MetALD spectrum[90].
GLP-1RAs have been repurposed for patients with MetALD. Its safety has been well-established in both MASLD and AUD. Adverse effects are predominantly related to the GI tract, including nausea, vomiting, constipation, gastroparesis, and possibly gallbladder-associated adverse effects[91]. Further, the GI side effects of GLP-1RA can potentially compound similar manifestations due to ongoing alcohol use. This potential interaction remains unstudied, and warrants caution when prescribing. It should also be recognized that 30%-40% of weight loss is lean body mass and muscle. This is especially relevant in older individuals and patients with cirrhosis, with a risk of obese sarcopenia in those with MASH. In a phase 2 trial, patients receiving semaglutide alone showed a 7.4% reduction in lean mass, compared with 2.9% in patients receiving adjuvant bimagrumab, a monoclonal antibody targeting type II activin receptors and stimulating muscle growth (P < 0.001). Similarly, preliminary results from the phase 2 COURAGE trial (NCT06299098) showed that the combination of trevogrumab, an anti-myostatin antibody, with semaglutide reduced lean mass loss by about 50%[92]. There were no safety concerns in either study.
Use of GLP-1 agonists requires caution in older adults and patients with cirrhosis, because loss of lean body mass may worsen sarcopenia. Agents targeting de novo lipogenesis, such as firsocostat, have shown limited efficacy and have been associated with pruritus and nausea, raising additional tolerability concerns in MetALD[44,93]. FXR-based therapy also warrants caution, given the experience with obeticholic acid, which was associated with severe pruritus, an adverse lipid profile, and serious liver-related safety concerns in clinical use, leading to its discontinuation in 2025.
Combining pharmacotherapy for CMRF with FDA-approved MAUD therapy may increase the risk of drug-drug interactions and require closer monitoring. In general, acamprosate is safe in patients with ALD. Naltrexone is metabolized in the liver and carries a black box warning for use in patients with decompensated liver disease, which was removed by the FDA in 2013 (https://www.fda.gov/safety/medical-product-safety-information/drug-safety-related-labeling-changes)[94,95]. Emerging retrospective data suggest that naltrexone may be safe in patients with ALD, including those with cirrhosis. Studies have reported improvements in liver enzymes, lower mortality, and fewer cases of hepatic decompensation among treated patients. In a large Veterans Administration (VA) cohort of patients with cirrhosis and prior decompensation, naltrexone showed an acceptable safety profile[95]. For practicing providers, we suggest that naltrexone can be used in patients with ALD without cirrhosis and those with compensated cirrhosis. However, it should be avoided in patients with decompensation, especially those with Child C cirrhosis. Close monitoring is recommended using liver chemistries and clinical evaluation, with the first evaluation at 2-4 weeks after starting naltrexone. The drug should be discontinued if the liver enzymes increase > 3× ULN, bilirubin gets elevated, or a decompensation event develops. Although baclofen, gabapentin, and topiramate lack significant hepatic metabolism, these drugs require dose adjustment based on renal function.
CONCLUSION
MetALD represents a major unmet need in hepatology, and current management relies largely on extrapolation from separate MASLD/MASH and ALD trials that systematically excluded patients with overlapping metabolic dysfunction and clinically meaningful alcohol exposure. Among emerging therapeutic candidates, GLP-1 receptor agonists and FGF21 analogs appear particularly promising due to their metabolic and antifibrotic benefits, along with a potential for improving alcohol-related behavior. Future MetALD-specific clinical trials should focus on (a) a study population characterized using self-reported alcohol use information complemented by alcohol biomarkers like phosphatidylethanol (PEth); (b) stratification by alcohol exposure, fibrosis stage, and cardiometabolic burden; (c) incorporate integrated liver, alcohol use, metabolic, clinical, and patient-centered outcomes, with focus on validating these end-points in this specific disease; and (d) recruitment and retention strategies.
DECLARATIONS
Authors’ contributions
Conceptualization, project administration, writing, review and editing, tables and figures: Pagadala M
Writing, review, editing, and investigation: Jalil S
Writing, investigation: Dunn N
Project supervision, validation, critical review, and editing: Singal AK
All authors approved the final version of the article, including the authorship list.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool NotebookLM was used solely for the preparation of the Graphical Abstract. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This study was supported by Kentucky Medicaid (SUP26-C5531), the National Institutes of Health (NIH; P20 GM103436 supplement), and the National Institute on Alcohol Abuse and Alcoholism (NIAAA; U01 AA026980-06) awarded to Singal AK.
Conflicts of interest
Singal AK serves as a consultant on the SBIR grant for Pleiogenix pharma; served as DSMB member for phase-2b DUR-928 trial for Durect pharma; serves on advisory board for Orphalan and Disc Medicine; Speaks and writes for Medscape, CLD Foundation, Expert Perspectives, Gastro Endo News, Dynamed, Medical Education Speakers Network, Up-to-Date, Madrigal Pharma, Practice Point. Singal AK is an Editorial Board Member of the journal Metabolism and Target Organ Damage. Singal AK was not involved in any steps of editorial processing, notably including reviewers’ selection, manuscript handling and decision making. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Rinella ME, Lazarus JV, Ratziu V, et al.; NAFLD Nomenclature consensus group. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79:1542-56.
2. Dunn N, Al-Khouri N, Abdellatif I, et al. Metabolic dysfunction and alcohol-associated liver disease: a narrative review. Clin Transl Gastroenterol. 2025;16:e00828.
3. Kalligeros M, Vassilopoulos A, Vassilopoulos S, Victor DW, Mylonakis E, Noureddin M. Prevalence of steatotic liver disease (MASLD, MetALD, and ALD) in the United States: NHANES 2017-2020. Clin Gastroenterol Hepatol. 2024;22:1330-2.e4.
4. Lee BP, Dodge JL, Terrault NA. National prevalence estimates for steatotic liver disease and subclassifications using consensus nomenclature. Hepatology. 2024;79:666-73.
5. Dunn N, Zhang W, Blaney HL, et al. Physical activity and advanced fibrosis in MASLD, MetALD, and ALD in a nationally representative cohort: NHANES 2017-2020. Hepatol Commun. 2025;9:e0797.
6. Kwak M, Kim HS, Jiang ZG, et al. MASLD/MetALD and mortality in individuals with any cardio-metabolic risk factor: a population-based study with 26.7 years of follow-up. Hepatology. 2025;81:228-37.
7. Elmustafa F, Tyagi M, Kaur H, et al. Met-ALD and ALD- does differentiating these impact management and clinical outcomes? Curr Hepatol Rep. 2025;24:10.1007/s11901-025.
8. Hagström H, Hegmar H, Moreno C. Interactions between the metabolic syndrome and alcohol consumption increases the risk of liver disease. United European Gastroenterol J. 2024;12:168-76.
9. Singal AK, Mathurin P. Diagnosis and treatment of alcohol-associated liver disease: a review. JAMA. 2021;326:165-76.
10. Francque SM, van der Graaff D, Kwanten WJ. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications. J Hepatol. 2016;65:425-43.
11. Åberg F, Färkkilä M. Drinking and obesity: alcoholic liver disease/nonalcoholic fatty liver disease interactions. Semin Liver Dis. 2020;40:154-62.
12. Wong VW, Chan RS, Wong GL, et al. Community-based lifestyle modification programme for non-alcoholic fatty liver disease: a randomized controlled trial. J Hepatol. 2013;59:536-42.
13. Keating SE, Chawla Y, De A, George ES. Lifestyle intervention for metabolic dysfunction-associated fatty liver disease: a 24-h integrated behavior perspective. Hepatol Int. 2024;18:959-76.
14. Bernardino M, Tiribelli C, Rosso N. The impact of the mediterranean diet, physical activity, and nutrition education on pediatric metabolic dysfunction-associated steatotic liver disease (MASLD): a review. Nutrients. 2025;18:28.
15. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77:1797-835.
16. Yeoh A, Wong R, Singal AK. The role bariatric surgery and endobariatric therapies in nonalcoholic steatohepatitis. Clin Liver Dis. 2023;27:413-27.
17. Hwang J, Hwang H, Shin H, et al. Bariatric intervention improves metabolic dysfunction-associated steatohepatitis in patients with obesity: a systematic review and meta-analysis. Clin Mol Hepatol. 2024;30:561-76.
18. Abdallah M, Brown L, Provenza J, Tariq R, Gowda S, Singal AK. Safety and efficacy of dyslipidemia treatment in NAFLD patients: a meta-analysis of randomized controlled trials. Ann Hepatol. 2022;27:100738.
19. Harrison SA, Bedossa P, Guy CD, et al.; MAESTRO-NASH investigators. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390:497-509.
20. Sanyal AJ, Newsome PN, Kliers I, et al.; ESSENCE Study Group. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. N Engl J Med. 2025;392:2089-99.
21. Singal AK, Wong RJ, Dasarathy S, et al. ACG clinical guideline: malnutrition and nutritional recommendations in liver disease. Am J Gastroenterol. 2025;120:950-72.
22. Gratacós-Ginès J, Ariño S, Sancho-Bru P, Bataller R, Pose E. MetALD: clinical aspects, pathophysiology and treatment. JHEP Rep. 2025;7:101250.
23. Patel S, Blaney H, Nassar S, Singal AK. GLP-1 receptor agonists and alcohol use disorder: a systematic review. Alcohol Alcohol. 2025;61:agaf069.
24. Tanguturi Yella SS, Kota Sesha Brahma Sree KS, Mahato SK. The role of glucagon-like peptide-1 receptor agonists in the treatment of alcohol use disorder: current evidence and future directions. J Clin Psychopharmacol. 2025;45:372-5.
25. van Bloemendaal L, Veltman DJ, Ten Kulve JS, et al. Brain reward-system activation in response to anticipation and consumption of palatable food is altered by glucagon-like peptide-1 receptor activation in humans. Diabetes Obes Metab. 2015;17:878-86.
26. Loomba R, Hartman ML, Lawitz EJ, et al.; SYNERGY-NASH Investigators. Tirzepatide for metabolic dysfunction-associated steatohepatitis with liver fibrosis. N Engl J Med. 2024;391:299-310.
27. Newsome PN, Sanyal AJ, Engebretsen KA, et al. Semaglutide 2.4 mg in participants with metabolic dysfunction-associated steatohepatitis: baseline characteristics and design of the phase 3 ESSENCE trial. Aliment Pharmacol Ther. 2024;60:1525-33.
28. Newsome PN, Ambery P. Incretins (GLP-1 receptor agonists and dual/triple agonists) and the liver. J Hepatol. 2023;79:1557-65.
29. Fisher FM, Maratos-Flier E. Understanding the physiology of FGF21. Annu Rev Physiol. 2016;78:223-41.
30. Meroni M, Dongiovanni P, Tiano F, Piciotti R, Alisi A, Panera N. β-Klotho as novel therapeutic target in metabolic dysfunction-associated steatotic liver disease (MASLD): a narrative review. Biomed Pharmacother. 2024;180:117608.
31. Harrison SA, Rolph T, Knott M, Dubourg J. FGF21 agonists: an emerging therapeutic for metabolic dysfunction-associated steatohepatitis and beyond. J Hepatol. 2024;81:562-76.
32. Rose JP, Morgan DA, Sullivan AI, et al. FGF21 reverses MASH through coordinated actions on the CNS and liver. Cell Metab. 2025;37:1515-29.e6.
33. Harrison SA, Ruane PJ, Freilich B, et al. A randomized, double-blind, placebo-controlled phase IIa trial of efruxifermin for patients with compensated NASH cirrhosis. JHEP Rep. 2023;5:100563.
34. Jeong C, Han N, Jeon N, et al. Efficacy and safety of fibroblast growth factor-21 analogs for the treatment of metabolic dysfunction-associated steatohepatitis: a systematic review and meta-analysis. Clin Pharmacol Ther. 2024;116:72-81.
35. Staels B, Butruille L, Francque S. Treating NASH by targeting peroxisome proliferator-activated receptors. J Hepatol. 2023;79:1302-16.
36. Results from the 52-week phase 2b VOYAGE trial of VK2809 in patients with biopsy-confirmed non-alcoholic steatohepatitis and fibrosis: a randomized, placebo-controlled trial. Gastroenterol Hepatol. 2024;20:13-4.
37. Kamata S, Honda A, Ishii I. Current clinical trial status and future prospects of PPAR-targeted drugs for treating nonalcoholic fatty liver disease. Biomolecules. 2023;13:1264.
38. Goyal O, Nohria S, Goyal P, et al. Saroglitazar in patients with non-alcoholic fatty liver disease and diabetic dyslipidemia: a prospective, observational, real world study. Sci Rep. 2020;10:21117.
39. Siddiqui MS, Parmar D, Sheikh F, et al. Saroglitazar, a dual PPAR α/γ agonist, improves atherogenic dyslipidemia in patients with non-cirrhotic nonalcoholic fatty liver disease: a pooled analysis. Clin Gastroenterol Hepatol. 2023;21:2597-605.e2.
40. Takahashi H, Kessoku T, Kawanaka M, et al. Ipragliflozin improves the hepatic outcomes of patients with diabetes with NAFLD. Hepatol Commun. 2022;6:120-32.
41. Jin Z, Yuan Y, Zheng C, Liu S, Weng H. Effects of sodium-glucose co-transporter 2 inhibitors on liver fibrosis in non-alcoholic fatty liver disease patients with type 2 diabetes mellitus: an updated meta-analysis of randomized controlled trials. J Diabetes Complications. 2023;37:108558.
43. Venetsanaki V, Karabouta Z, Polyzos SA. Farnesoid X nuclear receptor agonists for the treatment of nonalcoholic steatohepatitis. Eur J Pharmacol. 2019;863:172661.
44. Loomba R, Noureddin M, Kowdley KV, et al.; for the ATLAS Investigators. Combination therapies including cilofexor and firsocostat for bridging fibrosis and cirrhosis attributable to NASH. Hepatology. 2021;73:625-43.
45. Sanyal AJ, Lopez P, Lawitz EJ, et al. Tropifexor for nonalcoholic steatohepatitis: an adaptive, randomized, placebo-controlled phase 2a/b trial. Nat Med. 2023;29:392-400.
46. Ratziu V, Harrison SA, Loustaud-Ratti V, et al. Hepatic and renal improvements with FXR agonist vonafexor in individuals with suspected fibrotic NASH. J Hepatol. 2023;78:479-92.
47. Esler WP, Cohen DE. Pharmacologic inhibition of lipogenesis for the treatment of NAFLD. J Hepatol. 2024;80:362-77.
48. Loomba R, Bedossa P, Grimmer K, et al. Denifanstat for the treatment of metabolic dysfunction-associated steatohepatitis: a multicentre, double-blind, randomised, placebo-controlled, phase 2b trial. Lancet Gastroenterol Hepatol. 2024;9:1090-100.
49. Calle RA, Amin NB, Carvajal-Gonzalez S, et al. ACC inhibitor alone or co-administered with a DGAT2 inhibitor in patients with non-alcoholic fatty liver disease: two parallel, placebo-controlled, randomized phase 2a trials. Nat Med. 2021;27:1836-48.
50. Vujkovic M, Ramdas S, Lorenz KM, et al.; Regeneron Genetics Center, Geisinger-Regeneron DiscovEHR Collaboration, EPoS Consortium, VA Million Veteran Program. A multiancestry genome-wide association study of unexplained chronic ALT elevation as a proxy for nonalcoholic fatty liver disease with histological and radiological validation. Nat Genet. 2022;54:761-71.
51. Stickel F, Lutz P, Buch S, et al. Genetic variation in HSD17B13 reduces the risk of developing cirrhosis and hepatocellular carcinoma in alcohol misusers. Hepatology. 2020;72:88-102.
52. Schwantes-An TH, Darlay R, Mathurin P, et al.; GenomALC Consortium. Genome-wide association study and meta-analysis on alcohol-associated liver cirrhosis identifies genetic risk factors. Hepatology. 2021;73:1920-31.
53. Francque SM, Bedossa P, Ratziu V, et al.; NATIVE Study Group. A randomized, controlled trial of the Pan-PPAR agonist lanifibranor in NASH. N Engl J Med. 2021;385:1547-58.
54. Sanyal AJ, Bedossa P, Fraessdorf M, et al.; 1404-0043 Trial Investigators. A phase 2 randomized trial of survodutide in MASH and fibrosis. N Engl J Med. 2024;391:311-9.
55. Groenewegen B, Ruissen MM, Crossette E, et al. Consecutive fecal microbiota transplantation for metabolic dysfunction-associated steatotic liver disease: a randomized controlled trial. Gut Microbes. 2025;17:2541035.
56. Bajaj JS. Alcohol, liver disease and the gut microbiota. Nat Rev Gastroenterol Hepatol. 2019;16:235-46.
57. Witkiewitz K, Litten RZ, Leggio L. Advances in the science and treatment of alcohol use disorder. Sci Adv. 2019;5:eaax4043.
58. Anton RF, O’Malley SS, Ciraulo DA, et al.; COMBINE Study Research Group. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. 2006;295:2003-17.
59. Marek GW, Malhi H. MetALD: does it require a different therapeutic option? Hepatology. 2024;80:1424-40.
60. Kranzler HR, Soyka M. Diagnosis and pharmacotherapy of alcohol use disorder: a review. JAMA. 2018;320:815-24.
61. McPheeters M, O’Connor EA, Riley S, et al. Pharmacotherapy for alcohol use disorder: a systematic review and meta-analysis. JAMA. 2023;330:1653-65.
62. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of alcohol-related liver disease. J Hepatol. 2018;69:154-81.
63. Wu T, Mousa OY, Kulai T, et al. Safety of acamprosate in patients with alcohol-associated liver disease: a single-arm phase 2 trial. Mayo Clin Proc. 2025;100:954-61.
64. Leggio L, Hendershot CS, Farokhnia M, et al. GLP-1 receptor agonists are promising but unproven treatments for alcohol and substance use disorders. Nat Med. 2023;29:2993-5.
65. Wang W, Volkow ND, Berger NA, Davis PB, Kaelber DC, Xu R. Associations of semaglutide with incidence and recurrence of alcohol use disorder in real-world population. Nat Commun. 2024;15:4548.
66. Quddos F, Hubshman Z, Tegge A, et al. Semaglutide and tirzepatide reduce alcohol consumption in individuals with obesity. Sci Rep. 2023;13:20998.
67. Nasrollahizadeh A, Kheiri G, Javankiani S, et al. Repurposing GLP-1 receptor agonists for alcohol use disorder: a systematic review and meta-analysis. Diabetol Metab Syndr. 2026;18:29.
68. Cooley BJ, Occelli Hanbury-Brown CV, Choi EA, et al. FGF21 analogue PF-05231023 on alcohol consumption and neuronal activity in the nucleus accumbens. Neuropsychopharmacology. 2026;51:519-29.
69. Desai BN, Singhal G, Watanabe M, et al. Fibroblast growth factor 21 (FGF21) is robustly induced by ethanol and has a protective role in ethanol associated liver injury. Mol Metab. 2017;6:1395-406.
70. Flippo KH, Trammell SAJ, Gillum MP, et al. FGF21 suppresses alcohol consumption through an amygdalo-striatal circuit. Cell Metab. 2022;34:317-28.e6.
71. Cronjé HT, Hu S, Gurrell R, et al. Robust human genetic evidence supporting causal effects of FGF21 on reducing alcohol consuming behaviours. medRxiv 2025;2025.11.15.25340305v1. Available from: https://www.medrxiv.org/content/10.1101/2025.11.15.25340305v1.full. [Last accessed on 12 Jun 2026].
72. Shahi A, Yadav A, Rajak S, et al. Liver-specific thyroid hormone receptor-β agonism alleviates alcoholic steatohepatitis (ASH) in mice. Biochem Biophys Res Commun. 2024;734:150742.
73. Matheson J, Le Foll B. Therapeutic potential of peroxisome proliferator-activated receptor (PPAR) agonists in substance use disorders: a synthesis of preclinical and human evidence. Cells. 2020;9:1196.
74. Ferguson LB, Most D, Blednov YA, Harris RA. PPAR agonists regulate brain gene expression: relationship to their effects on ethanol consumption. Neuropharmacology. 2014;86:397-407.
75. Schwandt ML, Diazgranados N, Umhau JC, Kwako LE, George DT, Heilig M. PPARγ activation by pioglitazone does not suppress cravings for alcohol, and is associated with a risk of myopathy in treatment seeking alcohol dependent patients: a randomized controlled proof of principle study. Psychopharmacology. 2020;237:2367-80.
76. Karahanian E, Quintanilla ME, Fernandez K, Israel Y. Fenofibrate--a lipid-lowering drug--reduces voluntary alcohol drinking in rats. Alcohol. 2014;48:665-70.
77. Blednov YA, Benavidez JM, Black M, et al. Peroxisome proliferator-activated receptors α and γ are linked with alcohol consumption in mice and withdrawal and dependence in humans. Alcohol Clin Exp Res. 2015;39:136-45.
78. Rivera-Meza M, Muñoz D, Jerez E, et al. Fenofibrate administration reduces alcohol and saccharin intake in rats: possible effects at peripheral and central levels. Front Behav Neurosci. 2017;11:133.
79. Mutlu EA, Gillevet PM, Rangwala H, et al. Colonic microbiome is altered in alcoholism. Am J Physiol Gastrointest Liver Physiol. 2012;302:G966-78.
80. Wang SC, Chen YC, Chen SJ, Lee CH, Cheng CM. Alcohol addiction, gut microbiota, and alcoholism treatment: a review. Int J Mol Sci. 2020;21:6413.
81. Vatsalya V, Feng W, Kong M, et al. The beneficial effects of Lactobacillus GG therapy on liver and drinking assessments in patients with moderate alcohol-associated hepatitis. Am J Gastroenterol. 2023;118:1457-60.
82. Bajaj JS, Gavis EA, Fagan A, et al. A randomized clinical trial of fecal microbiota transplant for alcohol use disorder. Hepatology. 2021;73:1688-700.
83. Yu L, Wang L, Yi H, Wu X. Beneficial effects of LRP6-CRISPR on prevention of alcohol-related liver injury surpassed fecal microbiota transplant in a rat model. Gut Microbes. 2020;11:1015-29.
84. Arab JP, Díaz LA, Rehm J, et al. Metabolic dysfunction and alcohol-related liver disease (MetALD): position statement by an expert panel on alcohol-related liver disease. J Hepatol. 2025;82:744-56.
85. Gao B, Arab JP, Liangpunsakul S, et al. Metabolic dysfunction and alcohol-associated liver disease (MetALD). eGastroenterology. 2025;3:e100319.
86. Tampaki M, Tsochatzis E, Lekakis V, Cholongitas E. Prevalence, characteristics and outcomes of patients with metabolic and alcohol related/associated liver disease (MetALD): a systematic review and meta-analysis. Metabolism. 2025;163:156101.
87. Liu H, Lefere S, Guillot A, Zheng MH, Tacke F. Bariatric surgery for metabolic dysfunction-associated steatotic liver disease (MASLD): current knowledge of mechanisms. Hepatology. 2025;Epub ahead of print.
88. Singal AK, Leggio L, DiMartini A. Alcohol use disorder in alcohol-associated liver disease: two sides of the same coin. Liver Transpl. 2024;30:200-12.
89. Rady ED, Cotter TG. Integrating phosphatidylethanol to enhance alcohol quantification in steatotic liver disease and clinical trials. Liver Int. 2026;46:e70489.
90. Harrison SA, Schattenberg JM, Taub R, Labriola D. SAT-263 resmetirom treatment of a subgroup of patients with possible MetALD enrolled in MAESTRO-NASH, a phase 3 NASH/MASH serial liver biopsy study. J Hepatol. 2024;80:S141-2.
91. Sodhi M, Rezaeianzadeh R, Kezouh A, Etminan M. Risk of gastrointestinal adverse events associated with glucagon-like peptide-1 receptor agonists for weight loss. JAMA. 2023;330:1795-7.
92. Heymsfield SB, Aronne LJ, Montgomery P, et al. Bimagrumab plus semaglutide alone or in combination for the treatment of obesity: a randomized phase 2 trial. Nat Med. 2026;32:869-82.
93. Neokosmidis G, Cholongitas E, Tziomalos K. Acetyl-CoA carboxylase inhibitors in non-alcoholic steatohepatitis: is there a benefit? World J Gastroenterol. 2021;27:6522-6.
94. Niu C, Zhang J, Idoate-Domench DJ, et al. Evaluating the long-term benefits of medications for alcohol use disorder in alcohol-associated cirrhosis. Liver Int. 2025;45:e70424.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.