


History of gestational diabetes mellitus or hypertensive disorders of pregnancy and risk of chronic kidney disease
 0
0 
Abstract
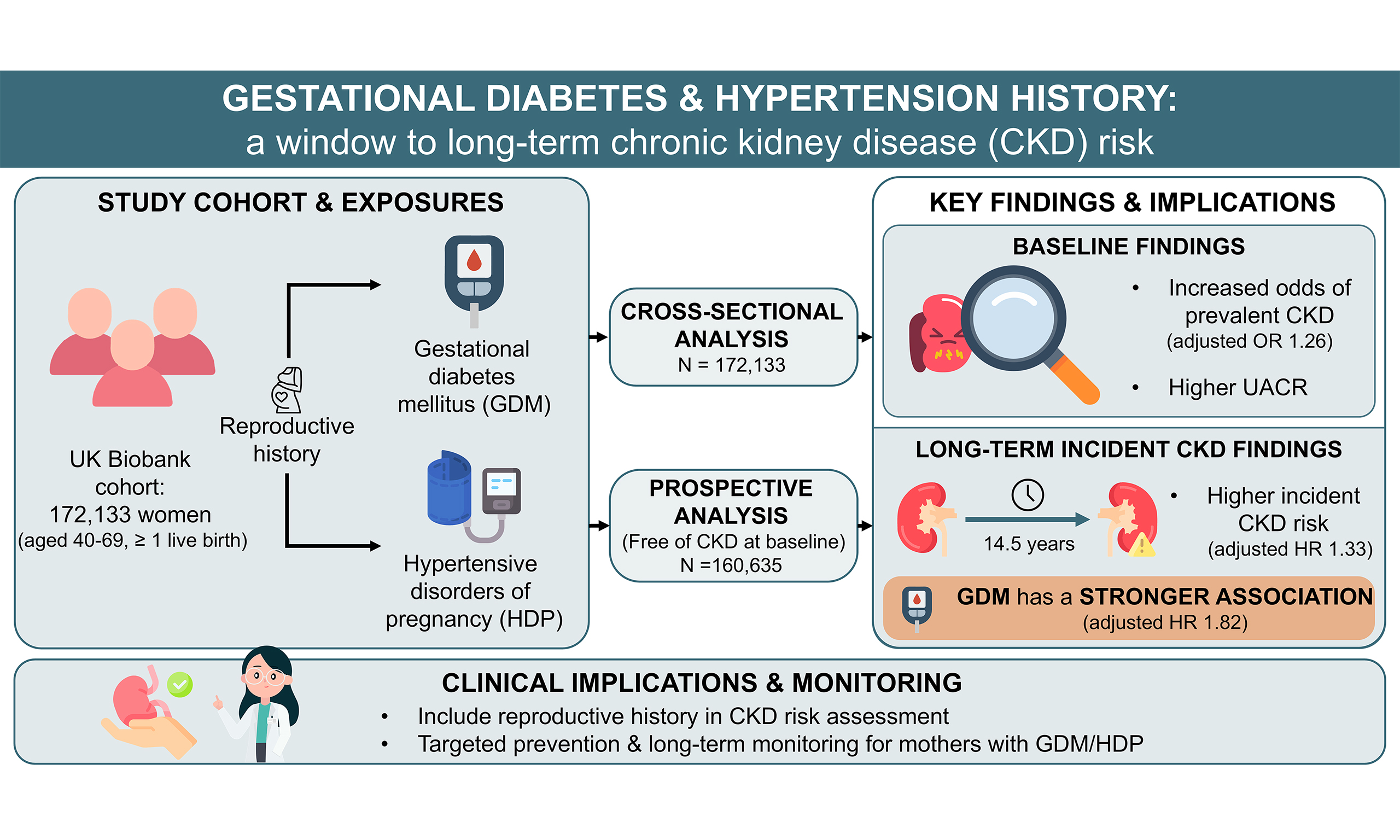
Aim: Chronic kidney disease (CKD) is a growing global concern, yet the long-term renal effects of gestational diabetes mellitus (GDM) and hypertensive disorders of pregnancy (HDP) remain unclear. This study evaluated the associations between GDM or HDP (GDM/HDP) history and CKD risk.
Methods: We used UK Biobank data to perform cross-sectional and prospective analyses. GDM and HDP were identified from self-reports or International Classification of Diseases, Tenth Revision (ICD-10) codes. Multivariable logistic, linear, and Cox regression models were used to assess associations with prevalent CKD and with renal function markers [estimated glomerular filtration rate (eGFR), urine albumin-to-creatinine ratio (UACR), urate, creatinine], and incident CKD, respectively.
Results: At baseline, 172,133 women were included in the cross-sectional analysis. Prior GDM/HDP was associated with a higher likelihood of prevalent CKD [odds ratio, 1.26; 95% confidence interval (CI): 1.11-1.43] and higher UACR; GDM was also associated with higher eGFR and lower urate and creatinine. In a prospective analysis of 160,635 women over a median follow-up of 14.5 years, GDM/HDP was associated with an increased incident risk of CKD [hazard ratio (HR), 1.33; 95%CI: 1.12-1.59]. GDM alone showed a stronger association with incident CKD (HR: 1.82; 95%CI: 1.39-2.40). In subgroup analyses, the associations of GDM/HDP, GDM, and HDP with incident CKD remained largely consistent across strata of age, body mass index (BMI), baseline eGFR, and major chronic conditions.
Conclusion: Prior GDM/HDP was associated with subsequent subclinical and clinical renal impairment, supporting the inclusion of reproductive history in CKD risk assessment and the need for targeted prevention and long-term monitoring.
Keywords
INTRODUCTION
The growing burden of chronic kidney disease (CKD) is a critical concern for global health systems, with the current age-standardized global prevalence estimated at 8.32%[1]. CKD is closely associated with the onset of end-stage renal failure and has been linked to an increased risk of adverse cardiovascular outcomes and premature mortality[2]. Furthermore, the impact of CKD extends beyond physical health, markedly diminishing health-related quality of life while placing a heavy financial strain on individuals and the healthcare system[3]. Therefore, identifying modifiable risk factors and early intervention strategies for CKD remains a public health priority.
Pregnancy complications may have lasting health effects on pregnant women. Gestational diabetes mellitus (GDM) is defined as glucose intolerance first recognized during pregnancy and is estimated to affect approximately 13%-17% of pregnancies worldwide[4]. Hypertensive disorders of pregnancy (HDP) encompass several severe clinical conditions, including preeclampsia, eclampsia, and gestational hypertension, which affect approximately 10% of pregnancies worldwide[5]. Both GDM and HDP are important risk factors for long-term metabolic dysfunction, particularly type 2 diabetes and cardiovascular disease (CVD)[6,7]. However, their potential long-term impact on renal health has been less studied. Accumulating evidence suggests that prior exposure to GDM or HDP (GDM/HDP) may increase susceptibility to CKD in later life[8-11]. Although several registry-based cohorts enrolled large populations, they failed to rigorously adjust for potential confounders[8,12,13]. In contrast, other studies have smaller sample sizes, typically ranging from 1,000 to 3,000 participants[14,15]. Given these methodological constraints, robust and large scale prospective research is essential to confirm the observed associations.
Utilizing data from the UK Biobank, this study performed both prospective and cross-sectional analyses to evaluate associations of prior GDM/HDP with CKD and diverse renal function indicators, including estimated glomerular filtration rate (eGFR), UACR, and serum urate and creatinine levels. This study provides robust epidemiological evidence to inform clinical practice and preventive strategies for individuals affected by prior pregnancy-related complications.
METHODS
Study design and population
Between 2006 and 2010, the UK Biobank recruited more than 500,000 community-dwelling adults (aged 40-69 years) across the country. This large-scale prospective cohort provides extensive longitudinal data, with follow-up through September 2023. At baseline, participants completed questionnaires covering sociodemographic factors, lifestyle and behaviors, environmental exposures, and medical history. These were supplemented by comprehensive physical assessments and biological sample collection[16,17]. To ensure comprehensive tracking, health outcomes are systematically updated by integrating multi-source datasets, such as primary care documentation, hospital episode statistics, outpatient registries, and national mortality records. The UK Biobank study received ethical approval from the North West Multi-Centre Research Ethics Committee (REC reference: 21/NW/0157, IRAS project ID: 299116), and all participants provided written informed consent. The present analyses were conducted under UK Biobank Application Number 103011 and required no additional institutional ethical approval because only de-identified data were used.
This study included women with at least one live birth at baseline and excluded those with missing parity information. To comprehensively assess the renal effects of adverse pregnancy outcomes, we performed both cross-sectional and prospective analyses. Participants with incomplete data on pregnancy complications or essential covariates were excluded [Supplementary Figure 1]. In the cross-sectional analysis, we investigated the association of prior GDM/HDP with the prevalence of CKD and with renal function markers measured at baseline. For the prospective analysis, we further excluded individuals with prevalent CKD at baseline to investigate the association between prior GDM/HDP and subsequent risk of incident CKD.
Assessment of exposures
A history of GDM/HDP was determined by integrating hospital inpatient records [International Classification of Diseases, Tenth Revision (ICD-10) codes; Supplementary Table 1] with baseline self-reports obtained through structured interviews or questionnaires[18]. This dual-ascertainment approach was used to capture cases across the full reproductive life course. Given their overlapping pathophysiology, we assessed these conditions both jointly and separately, defining the combined exposure as the primary exposure and the individual conditions as secondary exposures.
Assessment of outcomes
For the cross-sectional analysis, baseline CKD was defined either from hospital inpatient data, using ICD-10 diagnostic codes and the OPCS-4 (Office of Population Censuses and Surveys Classification of Interventions and Procedures, version 4) procedural codes[18] [Supplementary Table 1], or from laboratory markers, specifically an eGFR of less than 60 mL/min/1.73 m2 or a urine albumin-to-creatinine ratio (UACR) greater than 30 mg/g. Several commonly used renal function indices were also used as clinical endpoints, including eGFR, UACR, serum urate, and serum creatinine. We calculated the eGFR using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula, which accounts for serum creatinine levels, age, sex, and ethnicity[19]. We additionally derived cystatin C-based eGFR using the 2012 CKD-EPI cystatin C equation[20] to provide a filtration estimate less influenced by muscle mass and creatinine metabolism. UACR was calculated as the ratio of urinary albumin to creatinine, both of which were obtained from spot urine specimens[21]. Serum urate was measured using the uricase PAP method, and serum creatinine was measured enzymatically, both on Beckman Coulter AU5800 analyzers.
In the prospective analysis, the outcome was new-onset CKD. Incident CKD was identified using the same comprehensive approach as in the cross-sectional analysis, incorporating ICD-10 codes and relevant procedural and clinical codes[18] [Supplementary Table 1].
Assessment of covariates
Covariates assessed at baseline included sociodemographic factors, lifestyle and behaviors, reproductive history, laboratory measurements, and medication use. Sociodemographic and lifestyle variables included age, ethnicity (White or non-White), education (high: university degree or professional qualification; low: other qualifications), the Townsend deprivation index (an area-level proxy for socioeconomic status derived from residential postal codes[22]), body mass index (BMI), smoking status (current, former, or never), and alcohol consumption (daily, less than 14 units per week, special occasions only, or never). Parity was defined as the number of live births (1, 2, or ≥ 3 live births). Laboratory measurements at baseline were also included as covariates and quantified using standardized enzymatic or immunoturbidimetric assays on a Beckman Coulter AU5800 analyzer: triglycerides (enzymatic method), low-density lipoprotein cholesterol (LDL-C; enzymatic protective method), high-density lipoprotein cholesterol (HDL-C; enzyme-modified direct method), blood glucose (hexokinase method), and C-reactive protein (CRP; immunoturbidimetric assay)[23]. Baseline medication use, including antihypertensives and statins, was obtained via self-reports.
To enable subgroup stratification and mediation analyses, we assessed prevalent and incident major chronic conditions, including diabetes, hypertension, hyperlipidemia, and CVD. Baseline comorbidities were determined from a combination of self-reported data at enrollment and prior ICD codes [Supplementary Table 1]. Incident cases during follow-up were identified using ICD-10 codes.
Statistical analysis
Baseline characteristics of the study population were compared based on the history of GDM/HDP. Descriptive statistics are presented as means with SDs for continuous variables and as frequencies with corresponding percentages for categorical variables. Group differences were assessed using analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables.
To investigate the associations between the history of GDM/HDP and prevalent CKD at baseline, multivariable logistic regression models were used. We constructed three models to systematically adjust for potential confounders: Model 1 adjusted for age, ethnicity, education, and the Townsend deprivation index; Model 2 further adjusted for BMI, smoking status, and alcohol consumption; and Model 3 additionally adjusted for triglycerides, LDL-C, HDL-C, blood glucose, CRP, and medication use. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported for each model. To assess the relationship between GDM/HDP and continuous kidney function parameters (eGFR, UACR, urate, and creatinine), multivariable linear regression analyses were conducted, adjusting for all covariates included in Model 3. Standardized regression coefficients were visualized as heatmaps to illustrate association patterns between GDM/HDP and renal biomarkers.
In the prospective analysis, participants with prevalent CKD at baseline were excluded to ensure the identification of incident cases [Supplementary Figure 1]. Using Cox proportional hazards analysis, we estimated hazard ratios (HRs) with corresponding 95%CIs to assess the association between prior GDM/HDP and the risk of future CKD. These models applied the same stepwise covariate adjustment strategy as the cross-sectional analysis (Models 1-3), with baseline eGFR additionally included as a covariate in Model 3. To explore potential heterogeneity in these associations, we conducted stratified analyses across several key subgroups: age (≤ 60 years vs. > 60 years), BMI category (underweight/normal, < 24 kg/m2 vs. overweight/obesity, ≥ 24 kg/m2), baseline eGFR
Three types of sensitivity analyses were executed to verify that our core conclusions remained consistent. First, to minimize the potential impact of reverse bias, participants diagnosed with CKD during the initial 12 months of follow-up were removed from the repeat analysis. Second, we addressed data incompleteness by generating 10 imputed datasets using the chained equations approach, wherein continuous and dichotomous variables were imputed via predictive mean matching and logistic regression, respectively. Third, we additionally adjusted for parity to evaluate the robustness of the observed associations.
To explore the mechanistic pathways linking a history of GDM/HDP to incident CKD, we conducted mediation analyses within a time-dependent Cox proportional hazards framework. Four intermediate conditions (diabetes, hypertension, hyperlipidemia, and CVD) were treated as time-varying covariates to capture disease status over the follow-up period. Mediation effects were quantified using the difference-in-coefficients approach. Specifically, the total effect was estimated from a base Cox model adjusted for all covariates in Model 3, while the direct effect was obtained by additionally including each time-varying mediator. The indirect effect was defined as the difference between total and direct effects, while the mediated proportion was derived through the division of the indirect effect by the total effect. All 95%CIs and P values were derived from 1,000 bootstrap resamples.
We conducted all statistical procedures using R software (version 4.5.1). Unless noted otherwise, a two-tailed P value below 0.05 was the threshold for defining statistical significance.
RESULTS
Baseline characteristics
A total of 172,133 women were included in the cross-sectional analysis, of whom 1,070 had a history of GDM, and 2,509 had a history of HDP. The distribution of baseline characteristics for these participants is summarized in Supplementary Table 2. After excluding individuals with prevalent CKD at baseline, 160,635 women remained for the prospective analysis. Within this longitudinal cohort, 3,103 (1.93%) women had a documented history of GDM/HDP, including 968 with GDM and 2,313 with HDP; these conditions were not mutually exclusive. Women with prior GDM/HDP were younger at recruitment, had higher BMI, eGFR, and glucose levels, and were more likely to be non-White. They also had a higher prevalence of diabetes, hypertension, hyperlipidemia, and CVD [Table 1].
Baseline characteristics of women with and without a history of GDM/HDP in the UK Biobank in the prospective analysis
| Overall (N = 160,635) | Non-GDM/HDP (N = 157,419) | GDM/HDP (N = 3,216) | P valuea | |
| Age, mean (SD), years | 56.76 (7.82) | 56.85 (7.78) | 52.41 (8.51) | < 0.001 |
| BMI, mean (SD), kg/m2 | 27.01 (4.98) | 26.99 (4.96) | 28.22 (5.68) | < 0.001 |
| Ethnicity (White), n (%) | 154,309 (96.1) | 151,309 (96.1) | 3,000 (93.3) | < 0.001 |
| Education (High level), n (%) | 71,792 (44.7) | 70,195 (44.6) | 1,597 (49.7) | < 0.001 |
| Townsend deprivation index, mean (SD) | -1.57 (2.93) | -1.57 (2.93) | -1.45 (2.99) | 0.023 |
| Smoking status, n (%) | < 0.001 | |||
| Never | 97,719 (60.8) | 95,562 (60.7) | 2,157 (67.1) | |
| Previous | 52,167 (32.5) | 51,263 (32.6) | 904 (28.1) | |
| Current | 10,749 (6.7) | 10,594 (6.7) | 155 (4.8) | |
| Alcohol consumption, n (%) | < 0.001 | |||
| Special occasions only or never | 37,765 (23.5) | 36,932 (23.5) | 833 (25.9) | |
| Less than 14 units per week | 97,340 (60.6) | 95,345 (60.6) | 1,995 (62.0) | |
| Daily or almost daily | 25,530 (15.9) | 25,142 (16.0) | 388 (12.1) | |
| Clinical laboratory markers, mean (SD) | ||||
| eGFR, mL/min/1.73 m2 | 89.79 (11.47) | 89.73 (11.45) | 93.07 (12.22) | < 0.001 |
| UACR, mg/g | 8.35 (5.22) | 8.35 (5.21) | 8.34 (5.32) | 0.913 |
| Urate, mg/dL | 4.51 (1.06) | 4.51 (1.06) | 4.52 (1.09) | 0.507 |
| Creatinine, mg/dL | 0.72 (0.10) | 0.72 (0.10) | 0.71 (0.11) | 0.005 |
| Triglycerides, mg/dL | 137.55 (75.05) | 137.54 (74.94) | 137.89 (80.18) | 0.793 |
| LDL-C, mg/dL | 141.10 (33.50) | 141.23 (33.49) | 134.85 (33.47) | < 0.001 |
| HDL-C, mg/dL | 61.58 (14.34) | 61.62 (14.34) | 59.16 (14.33) | < 0.001 |
| Glucose, mg/dL | 90.86 (17.72) | 90.74 (17.29) | 96.44 (32.08) | < 0.001 |
| CRP, mg/dL | 0.26 (0.42) | 0.26 (0.42) | 0.28 (0.41) | 0.017 |
| Medication use, n (%) | ||||
| Antihypertensive drug | 27,271 (17.0) | 26,542 (16.9) | 729 (22.7) | < 0.001 |
| Statin | 19,738 (12.3) | 19,239 (12.2) | 499 (15.5) | < 0.001 |
| Diabetes, n (%) | 5,496 (3.4) | 4,620 (2.9) | 876 (27.2) | < 0.001 |
| Hypertension, n (%) | 35,699 (22.2) | 34,642 (22.0) | 1,057 (32.9) | < 0.001 |
| Hyperlipidemia, n (%) | 18,260 (11.4) | 17,845 (11.3) | 415 (12.9) | 0.006 |
| CVD, n (%) | 4,291 (2.7) | 4,193 (2.7) | 98 (3.0) | 0.200 |
Cross-sectional analysis
In the cross-sectional logistic regression analysis, women with prior GDM/HDP exhibited a significantly higher prevalence of CKD. After adjusting for age, ethnicity, education, and Townsend deprivation index in Model 1, prior GDM/HDP was associated with a higher likelihood of CKD (OR: 1.55; 95%CI: 1.37-1.76). The association remained robust after adjusting for additional covariates in Model 2 (OR: 1.47; 95%CI: 1.29-1.66) and remained significant in the fully adjusted Model 3 (OR: 1.26; 95%CI: 1.11-1.43), which additionally controlled for baseline laboratory markers and medication use. In addition, we separately analyzed the associations of GDM and HDP with prevalent CKD at baseline. In the fully adjusted model, a history of HDP was associated with significantly higher susceptibility to CKD (OR: 1.31; 95%CI: 1.12-1.52), whereas the association between GDM and CKD showed borderline significance (OR: 1.22; 95%CI: 0.98-1.50) [Table 2].
Cross-sectional association between GDM/HDP and CKD in the UK Biobank
| CKD/total (%) | Model 1 OR (95%CI)a | Model 2 OR (95%CI)b | Model 3 OR (95%CI)c | |
| GDM/HDP | ||||
| No | 7,679/168,629 (4.55%) | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 192/3,504 (5.48%) | 1.55 (1.37-1.76) | 1.47 (1.29-1.66) | 1.26 (1.11-1.43) |
| GDM | ||||
| No | 7,790/171,063 (4.55%) | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 81/1,070 (7.57%) | 1.82 (1.47-2.23) | 1.64 (1.32-2.01) | 1.22 (0.98-1.50) |
| HDP | ||||
| No | 7,755/169,624 (4.57%) | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 116/2,509 (4.62%) | 1.48 (1.27-1.71) | 1.42 (1.22-1.64) | 1.31 (1.12-1.52) |
In linear models, UACR was significantly higher among women with GDM/HDP, whether examined individually or jointly. In Model 3, the standardized β coefficients for UACR were 0.08 (95%CI: 0.05-0.11) for GDM/HDP, 0.12 (95%CI: 0.06-0.18) for GDM, and 0.07 (95%CI: 0.03-0.11) for HDP. For eGFR, only GDM alone showed a significant positive association in Model 3 (β = 0.08, 95%CI: 0.03-0.13). For serum urate and creatinine, GDM/HDP was not significantly associated with either marker, whereas GDM alone showed inverse associations with both markers in Model 3. Alongside elevated UACR, the combination of higher eGFR and lower serum creatinine may reflect early glomerular hyperfiltration, a feature of the early stages of diabetic kidney disease. Moreover, no significant differences were observed after recalculating eGFR using cystatin C-based equations [Figure 1 and Supplementary Table 3].
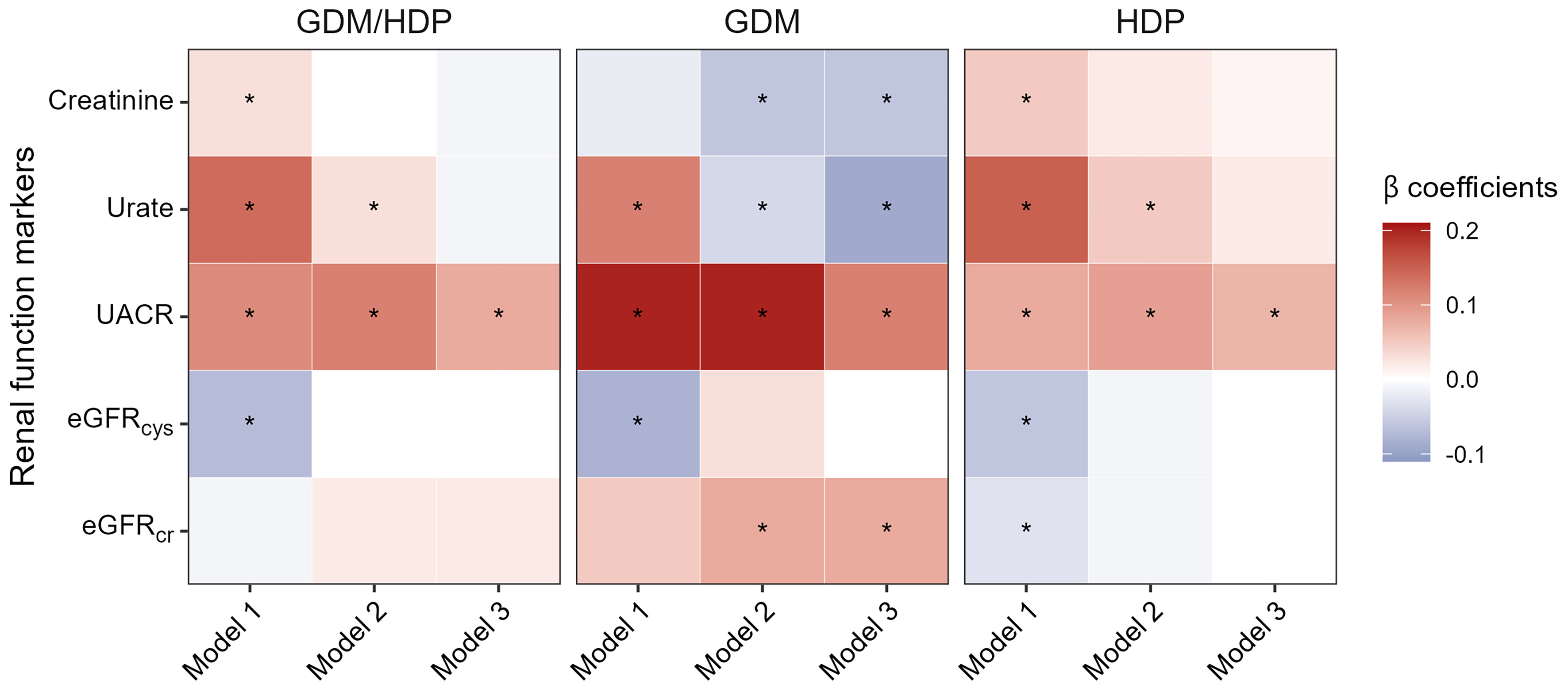
Figure 1. Associations between GDM/HDP and renal function markers in the UK Biobank in the cross-sectional analysis. Colors represent standardized β coefficients from linear regression models, with positive and negative associations highlighted in red and blue, respectively. All continuous variables were log2-transformed and standardized to z-scores before analysis. Asterisks within cells indicate statistical significance: *P < 0.05 after adjustment in Model 3. Model 1: adjusted for age, ethnicity, education, and Townsend deprivation index; Model 2: additionally adjusted for body mass index, smoking status, and alcohol consumption; Model 3: further adjusted for triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, blood glucose, C-reactive protein, and medication use. eGFRcr: Estimated glomerular filtration rate using creatinine; eGFRcys: estimated glomerular filtration rate using cystatin C; GDM: gestational diabetes mellitus; HDP: hypertensive disorders of pregnancy; UACR: urine albumin-to-creatinine ratio.
Prospective cohort analysis
During a median follow-up of 14.5 years, 5,602 incident CKD events were identified among 160,635 individuals in the study population. After full adjustment in the Cox proportional hazards model, prior GDM/HDP was associated with an increased risk of incident CKD (HR: 1.33, 95%CI: 1.12-1.59). We further examined the associations of GDM and HDP separately with incident CKD. Following comprehensive adjustment for all covariates, prior GDM remained significantly associated with increased CKD risk (HR: 1.82, 95%CI: 1.39-2.40), whereas no significant association was observed for HDP (HR: 1.14, 95%CI: 0.91-1.43) [Table 3].
Prospective associations between GDM/HDP and incident CKD in the UK Biobank
| CKD/person-years | Model 1a HR (95%CI) | Model 2b HR (95%CI) | Model 3c HR (95%CI) | |
| GDM/HDP | ||||
| No | 5,477/2,222,161 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 125/45,583 | 1.65 (1.38-1.97) | 1.50 (1.26-1.79) | 1.33 (1.12-1.59) |
| GDM | ||||
| No | 5,549/2,254,208 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 53/13,536 | 2.62 (2.00-3.43) | 2.18 (1.66-2.86) | 1.82 (1.39-2.40) |
| HDP | ||||
| No | 5,526/2,234,795 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 76/32,949 | 1.34 (1.07-1.68) | 1.26 (1.00-1.58) | 1.14 (0.91-1.43) |
Subgroup and sensitivity analyses
In subgroup analyses, the associations of GDM/HDP, GDM, and HDP with incident CKD remained largely consistent across strata of age, BMI, baseline eGFR, and major chronic conditions [Supplementary Table 4]. The associations of GDM/HDP and HDP alone with incident CKD were stronger among women with baseline eGFR ≤ 90 mL/min/1.73 m2, compared with those with eGFR > 90 mL/min/1.73 m2 (HR: 1.69 vs. 1.21 for GDM/HDP and 1.70 vs. 1.02 for HDP alone; P for interaction = 0.013 and 0.038, respectively; Supplementary Table 4). Furthermore, the association between GDM alone and CKD risk appeared to be stronger among women with hyperlipidemia (HR: 2.50 vs. 1.30; P for interaction = 0.008). However, after Benjamini-Hochberg false discovery rate (FDR) correction, the evidence for effect modification by eGFR and hyperlipidemia was attenuated to marginal significance. (FDR-adjusted P < 0.05 for all; Figure 2).
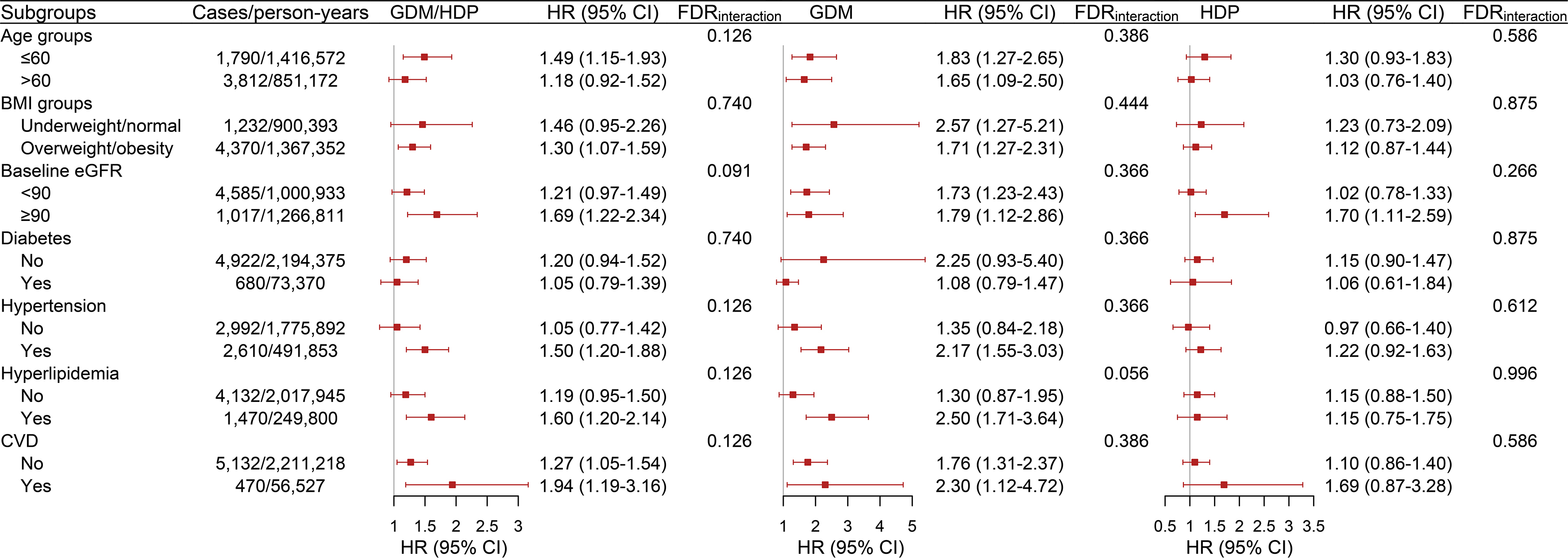
Figure 2. Associations between GDM/HDP and incident CKD across major subgroups in the UK Biobank. Models were adjusted for age, ethnicity, education, Townsend deprivation index, BMI, smoking status, alcohol consumption, eGFR, triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, blood glucose, C-reactive protein, and medication use. P values for interaction (i.e., FDRinteraction) were derived from likelihood ratio tests comparing nested models with and without cross-product terms between the stratifying variable and GDM/HDP status, and were adjusted for multiple testing using the Benjamini-Hochberg FDR method. BMI: Body mass index; CI: confidence interval; CKD: chronic kidney disease; CVD: cardiovascular disease; eGFR: estimated glomerular filtration rate; FDR: false discovery rate; GDM: gestational diabetes mellitus; HR: hazard ratio.
Sensitivity analyses yielded results consistent with those observed in the primary prospective analysis [Table 4 and Supplementary Table 5]. Excluding CKD cases occurring within one year of baseline did not materially alter the findings (HR for GDM/HDP: 1.34, 95%CI: 1.12-1.61; HR for GDM alone: 1.83, 95%CI: 1.39-2.42; HR for HDP alone: 1.16, 95%CI: 0.92-1.45). The findings remained consistent after addressing missing covariate data using multiple imputation (HR for GDM/HDP: 1.29, 95%CI: 1.09-1.53; HR for GDM alone: 1.78, 95%CI: 1.38-2.30; HR for HDP alone: 1.09, 95%CI: 0.87-1.36) and after further adjustment for parity.
Sensitivity analyses for associations between history of GDM/HDP and incident CKD
| CKD/person-years | Model 1a HR (95%CI) | Model 2b HR (95%CI) | Model 3c HR (95%CI) | |
| GDM/HDP | ||||
| Sensitivity analysis 1d | ||||
| No | 5,440/2,222,064 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 124/45,583 | 1.65 (1.38-1.97) | 1.50 (1.25-1.79) | 1.34 (1.12-1.61) |
| Sensitivity analysis 2e | ||||
| No | 7,061/2,857,482 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 158/60,146 | 1.57 (1.34-1.84) | 1.43 (1.22-1.68) | 1.29 (1.09-1.53) |
| GDM | ||||
| Sensitivity analysis 1d | ||||
| No | 5,512/2,254,112 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 52/13,536 | 2.59 (1.97-3.40) | 2.16 (1.64-2.84) | 1.83 (1.39-2.42) |
| Sensitivity analysis 2e | ||||
| No | 7,146/2,899,418 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 73/18,210 | 2.59 (2.06-3.26) | 2.14 (1.70-2.70) | 1.78 (1.38-2.30) |
| HDP | ||||
| Sensitivity analysis 1d | ||||
| No | 5,488/2,234,697 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 76/32,950 | 1.35 (1.08-1.70) | 1.27 (1.01-1.59) | 1.16 (0.92-1.45) |
| Sensitivity analysis 2e | ||||
| No | 7,130/2,874,457 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Yes | 89/43,171 | 1.20 (0.98-1.48) | 1.14 (0.93-1.41) | 1.09 (0.87-1.36) |
Mediation analysis
In mediation analyses, diabetes accounted for the largest proportion of the association between prior GDM/HDP and incident CKD (48.9%; 95%CI: 28.1%-100.0%). CVD and hypertension also contributed to the mediated effect, accounting for 13.5% (95%CI: 0.6%-48.4%) and 12.5% (95%CI: 5.8%-33.7%) of the total effect, respectively. Hyperlipidemia showed no evidence of mediation (0.8%; 95%CI: -3.9%-6.8%) [Table 5]. In separate analyses of GDM and HDP, diabetes remained a major mediator of the GDM-CKD association (67.6%; 95%CI: 44.1%-100%) [Supplementary Tables 6 and 7].
Major chronic conditions mediating the link between prior GDM/HDP and incident CKD
| Mediators | Indirect effect β (95%CI) | Direct effect β (95%CI) | Proportion mediated (95%CI) | P value |
| Diabetes | 0.147 (-0.045-0.323) | 0.141 (0.111-0.176) | 48.9% (28.1%-100%) | 0.002 |
| Hypertension | 0.252 (0.076-0.424) | 0.036 (0.019-0.054) | 12.5% (5.8%-33.7%) | 0.002 |
| Hyperlipidemia | 0.286 (0.102-0.461) | 0.002 (-0.008-0.015) | 0.8% (-3.9%-6.8%) | 0.662 |
| CVD | 0.249 (0.058-0.427) | 0.039 (0.002-0.073) | 13.5% (0.6%-48.4%) | 0.042 |
DISCUSSION
In this large UK Biobank cohort of more than 170,000 women, prior GDM/HDP was associated with subsequent CKD risk, with the association being stronger for GDM than for HDP. Both GDM and HDP were consistently associated with elevated UACR, while GDM was also associated with higher eGFR and lower serum urate and creatinine. The associations between prior GDM/HDP and incident CKD remained largely consistent across strata of age, BMI, baseline eGFR, and major chronic conditions. Our findings highlight the need to integrate pregnancy history into long-term renal health assessments for women.
A history of GDM has been identified as a significant risk factor for future CKD in the present cohort. This finding aligns with a large nationwide Danish cohort[8] and the CARDIA (Coronary Artery Risk Development in Young Adults) project[24], both of which reported that GDM was associated with increased long-term renal risk independent of traditional metabolic comorbidities. Although our cross-sectional analysis provided only limited evidence of an association between prior GDM and prevalent CKD, women with a history of GDM exhibited higher eGFR levels. This pattern could be consistent with early glomerular hyperfiltration, a phenomenon commonly observed in populations at high metabolic risk[25]. Initially compensatory, glomerular hyperfiltration in the setting of insulin resistance and hyperglycemia may become maladaptive over time, contributing to glomerular injury and increasing long-term CKD risk[26]. Similarly, the Diabetes & Women’s Health study reported higher eGFR levels in women with a history of GDM, consistent with our observations[27]. However, this interpretation should be viewed with caution. In a supplementary analysis, eGFR recalculated using cystatin C-based equations did not differ significantly by GDM history. Thus, the observed pattern of higher creatinine-based eGFR may not necessarily indicate glomerular hyperfiltration alone, but may reflect differences in creatinine generation, muscle mass, or measurement variability. Nevertheless, the consistent positive association between GDM and UACR suggests that GDM may be associated with early kidney alterations before overt loss of filtration function[28]. GDM was also inversely associated with serum urate and creatinine levels, highlighting altered renal handling or differences in metabolite generation in metabolic dysregulation. Further studies are needed to clarify the biological pathways linking GDM history to subsequent CKD risk.
Our findings suggest that HDP and GDM may differ in their associations with kidney outcomes over time. Although HDP was significantly associated with prevalent CKD, its association with incident CKD was attenuated in prospective analyses. This pattern suggests that GDM may serve as a more prominent marker of long-term kidney vulnerability in this cohort. This pattern does not negate the established role of HDP in kidney disease; rather, it is broadly consistent with prior large population-based studies linking HDP history to increased risks of CKD and advanced kidney disease[13,14,29-31]. Registry-based studies in Denmark, Spain, and Sweden leveraged exceptionally large sample sizes[13,29,32]; however, reliance on nationwide registries introduces important limitations, including limited clinical detail, non-standardized follow-up, and incomplete control for confounding. Whereas these prior studies have focused on preeclampsia, our study examined the broader spectrum of HDP, including gestational hypertension, chronic hypertension, preeclampsia/eclampsia, and preeclampsia superimposed on chronic hypertension. This broader case definition allowed us to more comprehensively assess the long-term kidney risk associated with HDP history. Similarly, a prospective cohort study from sub-Saharan Africa reported that women with HDP were more likely to have decreased eGFR postpartum, with the highest risk observed among those with preeclampsia/eclampsia[14]. A cross-sectional study conducted 10 years postpartum found that prior preeclampsia was associated with a subtle shift toward higher-normal eGFR values and a slight increase in proteinuria[33]. Consistent with these findings, our cross-sectional results showed a marked positive correlation linking HDP to UACR; notably, no such association was observed with eGFR. This disparity underscores the potential for albuminuria-related indices to detect early renal deviations following HDP with greater sensitivity than fluctuations in the glomerular filtration rate.
The association between GDM/HDP history and later CKD risk may reflect persistent metabolic disturbances, endothelial dysfunction, and chronic inflammation after pregnancy, which could contribute to long-term renal impairment[34-36]. In GDM, chronic low-grade inflammation, insulin resistance, and hyperglycemia during pregnancy may induce glomerular hyperfiltration and increase oxidative stress, resulting in structural and functional changes in the kidney[24,34]. These metabolic disturbances may persist or worsen after pregnancy, particularly among women who later develop type 2 diabetes or metabolic syndrome, thereby increasing long-term CKD risk[35]. A history of GDM may significantly increase susceptibility to metabolic dysfunction among women, including hypertension and dyslipidemia, which could subsequently contribute to the long-term risk of CKD[11,37]. Our findings suggest that incident diabetes and hypertension partially mediated the association between GDM/HDP and subsequent CKD. For GDM alone, incident diabetes was the only time-varying condition that significantly mediated the association with CKD, whereas no significant mediation was observed for the other time-varying conditions. Nevertheless, these intermediate cardiometabolic states remain clinically relevant and should be considered in long-term kidney risk management for high-risk women. In HDP, particularly preeclampsia, endothelial dysfunction is a hallmark pathological feature that may contribute to systemic microvascular injury and glomerular endotheliosis during pregnancy[38]. Although these changes often resolve after delivery, accumulating evidence suggests that preeclampsia may leave persistent vascular and renal alterations, including residual glomerular damage, podocyte loss, and impaired renal blood flow autoregulation, which may predispose women to long-term renal dysfunction and increased CKD risk[39]. Additionally, HDP is associated with a higher risk of future hypertension and metabolic syndrome, both of which are major contributors to CKD. Overall, our findings underscore the importance of proactive screening and tailored risk management for women with previous HDP/GDM to prevent or delay the onset of CKD.
The large-scale cohort design, inclusion of multiple kidney-related endpoints, and comprehensive adjustment for relevant clinical and metabolic factors strengthen the robustness of our findings. Nevertheless, several limitations should be acknowledged. First, the healthy-volunteer bias inherent in the UK Biobank may have resulted in conservative estimates. Given that the UK Biobank likely represents a survivor-enriched population, the renal consequences of pregnancy complications may be underestimated. Retrospective self-reported reproductive history may also introduce recall error or exposure misclassification; however, such misclassification is expected to be non-differential, which typically dilutes the observed associations toward the null value. Second, the demographic homogeneity of the UK Biobank, which predominantly comprises relatively healthy White participants, may limit the generalizability of our findings to broader or more vulnerable populations with diverse racial/ethnic backgrounds, environmental exposures, or healthcare access. Third, the cross-sectional nature of biomarker measurements limits causal inference and does not capture dynamic changes in kidney function over time. Longitudinal studies with repeated biomarker profiling are needed to characterize renal trajectories and clarify the biological pathways linking pregnancy complications to later-life kidney disease. Fourth, data limitations precluded further subclassification of HDP and assessment of potential heterogeneity in kidney risk across distinct HDP subtypes. Fifth, information on several important maternal characteristics, such as BMI before pregnancy and weight gain during gestation, was not recorded in the UK Biobank. Although baseline metabolic markers were used as partial proxies, residual confounding cannot be excluded.
In summary, our findings suggest that a history of GDM/HDP may serve as an important marker of later-life kidney vulnerability, including both subclinical alterations and clinically evident CKD. These results underscore the need to integrate obstetric history into CKD risk assessment and to develop targeted surveillance and prevention strategies for women who have experienced pregnancy complications.
DECLARATIONS
Acknowledgments
This work uses data provided by patients and collected by the NHS as part of their care and support. The authors thank the participants and staff of the UK Biobank for their invaluable contributions.
Authors’ contributions
Conceptualization, methodology, and original draft preparation: Wang Y, Wu N, Yang Y, Pan XF
Data acquisition and curation: Wang Y, Wu N, Luo X, Li F, Zhao Y, He Q
Data analysis, interpretation, and visualization: Wang Y, Wu N, Pan XF
Validation and investigation: Zhang S, Dong Y, He X, Wang T, Li Y
Created new software used in the work: Wang Y, Wu N
Drafting of the manuscript: Wang Y, Wu N, Pan XF
Substantively revised the work for important intellectual content: Yang Y, Li R, Li S, Xue Q, Wen Y, Wu J
Administrative, technical, and material support, and overall supervision: Pan XF
All authors read and approved the final manuscript.
Availability of data and materials
The datasets are available upon reasonable request to the Access Management System (AMS) through the UK Biobank website (https://www.ukbiobank.ac.uk/use-our-data/apply-for-access).
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This study was sponsored by the National Natural Science Foundation of China (82473646). Li F was funded by the National Natural Science Foundation of China (62506250), China Postdoctoral Science Foundation (2024M762216), and Sichuan Provincial Natural Science Foundation (2025ZNSFSC1467). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of interest
Pan XF is the Guest Editor of the special issue entitled “Gestational Diabetes Mellitus: Mechanisms, Risk Prediction, and Long-Term Consequences” in the journal Metabolism and Target Organ Damage. Pan XF was not involved in any steps of editorial processing, notably including reviewers’ selection, manuscript handling and decision-making. The other authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
The UK Biobank study was approved by the North West Multi-center Research Ethics Committee (MREC; REC reference: 21/NW/0157; IRAS project ID: 299116), and all participants provided written informed consent prior to data collection. The present analysis was conducted under UK Biobank Application Number 103011 and required no additional institutional ethical approval because only de-identified data were used.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Global Burden of Disease Collaborative Network. GBD Results Tool. Institute for Health Metrics and Evaluation (IHME), Seattle, WA, 2024. Available from https://vizhub.healthdata.org/gbd-results/ [accessed 24 June 2026].
2. Lailler G, Grave C, Gabet A, et al. Early mortality, cardiovascular, and renal diseases in women’s lives following hypertensive disorders of pregnancy: the prospective nationwide study CONCEPTION. J Am Heart Assoc. 2024;13:e033252.
3. disease: improving global outcomes (KDIGO) diabetes work group. KDIGO 2022 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2022;102:S1-127.
4. Wang B, Wang N, Yin X, et al. Gestational diabetes mellitus and accelerated biological aging in middle-aged and elderly women. Diabetes Care. 2026;49:317-24.
5. Fan L, Ding L, Nie J, Wang J, Zhang M, Zhang J. Hypertensive disorders of pregnancy: a comprehensive review of pathophysiology, diagnosis, treatment, and long-term cardiovascular implications. Clin Exp Hypertens. 2026;48:2641542.
6. Kramer CK, Campbell S, Retnakaran R. Gestational diabetes and the risk of cardiovascular disease in women: a systematic review and meta-analysis. Diabetologia. 2019;62:905-14.
7. Wambua S, Singh M, Okoth K, et al.; MuM-PreDiCT Group. Association between pregnancy-related complications and development of type 2 diabetes and hypertension in women: an umbrella review. BMC Med. 2024;22:66.
8. Christensen MH, Bistrup C, Rubin KH, et al. Kidney disease in women with previous gestational diabetes mellitus: a nationwide register-based cohort study. Diabetes Care. 2024;47:401-8.
9. Piccoli GB, Torreggiani M, Schwotzer N, et al. Kidney health outcomes of hypertensive disorders of pregnancy. Nat Rev Nephrol. 2025;21:671-86.
10. Shapiro J, Ray JG, McArthur E, et al. Risk of acute kidney injury after hypertensive disorders of pregnancy: a population-based cohort study. Am J Kidney Dis. 2022;79:561-9.
11. Hamill M, Gomez Fernandez C, Mitsigiorgi R, Mansukhani T, Nicolaides KH, Bramham K. Kidney dysfunction following gestational diabetes mellitus. Clin J Am Soc Nephrol. 2025;20:1418-26.
12. Barrett PM, McCarthy FP, Evans M, et al. Hypertensive disorders of pregnancy and the risk of chronic kidney disease: a Swedish registry-based cohort study. PLoS Med. 2020;17:e1003255.
13. Khashan AS, Evans M, Kublickas M, et al. Preeclampsia and risk of end stage kidney disease: a Swedish nationwide cohort study. PLoS Med. 2019;16:e1002875.
14. Ishaku SM, Olanrewaju TO, Browne JL, et al. Prevalence and determinants of chronic kidney disease in women with hypertensive disorders in pregnancy in Nigeria: a cohort study. BMC Nephrol. 2021;22:229.
15. An U, Pazokitoroudi A, Alvarez M, et al. Deep learning-based phenotype imputation on population-scale biobank data increases genetic discoveries. Nat Genet. 2023;55:2269-76.
16. Allen NE, Lacey B, Lawlor DA, et al. Prospective study design and data analysis in UK Biobank. Sci Transl Med. 2024;16:eadf4428.
17. Jiang Y, Zhao B, Wang X, et al. UKB-MDRMF: a multi-disease risk and multimorbidity framework based on UK biobank data. Nat Commun. 2025;16:3767.
18. Heo GY, Koh HB, Park JT, et al. Sweetened beverage intake and incident chronic kidney disease in the UK biobank study. JAMA Netw Open. 2024;7:e2356885.
19. Levey AS, Stevens LA, Schmid CH, et al.; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604-12.
20. Inker LA, Schmid CH, Tighiouart H, et al.; CKD-EPI Investigators. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367:20-9.
21. Lamb EJ, MacKenzie F, Stevens PE. How should proteinuria be detected and measured? Ann Clin Biochem. 2009;46:205-17.
22. Townsend P, Phillimore P, Beattie A. Health and deprivation: inequality and the North. 1st ed. Abingdon: Routledge; 2023. Available from: https://www.taylorfrancis.com/books/mono/10.4324/9781003368885/health-deprivation-peter-townsend-peter-phillimore-alastair-beattie. [Last accessed on 8 Jun 2026].
23. Sun Y, Cao D, Zhang Y, et al. Appraising associations between signature lipidomic biomarkers and digestive system cancer risk: novel evidences from a prospective cohort study of UK Biobank and Mendelian randomization analyses. Lipids Health Dis. 2024;23:61.
24. Dehmer EW, Phadnis MA, Gunderson EP, et al. Association between gestational diabetes and incident maternal CKD: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Kidney Dis. 2018;71:112-22.
25. Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12:2032-45.
26. Cortinovis M, Perico N, Ruggenenti P, Remuzzi A, Remuzzi G. Glomerular hyperfiltration. Nat Rev Nephrol. 2022;18:435-51.
27. Rawal S, Olsen SF, Grunnet LG, et al. Gestational diabetes mellitus and renal function: a prospective study with 9- to 16-year follow-up after pregnancy. Diabetes Care. 2018;41:1378-84.
28. Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105:S117-314.
29. Abbate M, Parvanova A, López-González ÁA, et al. MAFLD and glomerular hyperfiltration in subjects with normoglycemia, prediabetes and type 2 diabetes: a cross-sectional population study. Diabetes Metab Res Rev. 2024;40:e3810.
30. Moriconi D. Glomerular hyperfiltration in diabesity: an overlooked target for early intervention. J Nephrol. 2026;39:76-9.
31. Zhang M, Liu WL, Xu G, Dong L. Hyperlipidemia in membranous nephropathy. Clin Kidney J. 2026;19:sfag032.
32. Wuttke M, Li Y, Li M, et al.; Lifelines Cohort Study, V. A. Million Veteran Program. A catalog of genetic loci associated with kidney function from analyses of a million individuals. Nat Genet. 2019;51:957-72.
33. Paauw ND, Joles JA, Drost JT, et al. High-normal estimated glomerular filtration rate in early-onset preeclamptic women 10 years postpartum. Hypertension. 2016;68:1407-14.
34. Tseng ST, Lee MC, Tsai YT, et al. Risks after gestational diabetes mellitus in taiwanese women: a nationwide retrospective cohort study. Biomedicines. 2023;11:2120.
35. Li Z, Cheng Y, Wang D, et al. Incidence rate of type 2 diabetes mellitus after gestational diabetes mellitus: a systematic review and meta-analysis of 170,139 women. J Diabetes Res. 2020;2020:3076463.
36. Sabayev M, Ganio EA, Stelzer IA, et al. Systemic immune dysregulation in hypertensive disorders of pregnancy persists years after delivery. Front Immunol. 2026;17:1716809.
37. Echouffo-Tcheugui JB, Tapia S, Bechraoui-Quantin S, et al. Gestational diabetes mellitus and incident kidney disease: a nationwide french cohort study. Kidney360. 2026;Epub ahead of print.
38. Herman RJ, Ambasta A, Williams RG, et al. Sequential measurement of the neurosensory retina in hypertensive disorders of pregnancy: a model of microvascular injury in hypertensive emergency. J Hum Hypertens. 2023;37:28-35.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.