


Osimertinib in EGFR-mutated non-small cell lung cancer: a comprehensive narrative review of clinical evidence
 0
0 Abstract
Osimertinib, a third-generation, mutant-selective, irreversible epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor, has fundamentally reshaped the treatment landscape of EGFR-mutated non-small cell lung cancer (NSCLC). Originally approved for T790M-positive disease after progression on earlier-generation tyrosine kinase inhibitors (TKIs), osimertinib has since become the standard-of-care first-line therapy for advanced EGFR exon 19 deletion/L858R-positive NSCLC and the first targeted adjuvant therapy in resected early-stage disease. Its superior systemic efficacy, favorable safety profile, and exceptional central nervous system (CNS) penetration distinguish it from all predecessor agents. However, inevitably acquired resistance, driven by heterogeneous on-target tertiary EGFR mutations, off-target bypass pathway activation, and histological transformation, remains the principal clinical challenge. The postosimertinib treatment era is now being shaped by mesenchymal-epithelial transition factor (MET)-targeted combinations, antibody-drug conjugates, EGFR-MET bispecific antibodies, fourth-generation EGFR TKIs, and frontline intensification strategies. This review synthesizes the current evidence on the clinical indications of osimertinib, efficacy and CNS control, resistance mechanisms and their line-dependent patterns, postprogression management algorithms, combination strategies, guideline evolution, and future directions, providing a comprehensive framework for clinical decision-making and research prioritization.
Keywords
INTRODUCTION
Lung cancer remains the leading cause of cancer-related mortality worldwide, and non-small cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer diagnoses[1]. The therapeutic landscape of cancer has undergone a profound transformation over the past two decades, evolving from empirical cytotoxic chemotherapy to molecularly targeted and immunologically driven strategies that exploit tumor-specific vulnerabilities. Among the molecularly defined subsets of NSCLC, tumors harboring activating mutations in the epidermal growth factor receptor (EGFR) gene exemplify this paradigm shift, principally exon 19 deletions (ex19del) and the exon 21 L858R point mutation, which represent a clinically distinct entity characterized by sensitivity to EGFR tyrosine kinase inhibitors (TKIs)[2-4]. The identification of these driver mutations and the subsequent development of genotype-directed therapies marked the advent of precision oncology in thoracic malignancies. First-generation (gefitinib, erlotinib) and second-generation (afatinib, dacomitinib) EGFR TKIs have demonstrated initial response rates of 60% to 70%, yet acquired resistance invariably develops within 9 to 14 months, with the EGFR T790M gatekeeper mutation accounting for approximately 50% to 60% of resistance cases[5-10]. This unmet clinical need has led to the development of osimertinib (AZD9291, Tagrisso™), a third-generation EGFR TKI selectively designed to inhibit both EGFR-sensitizing mutations and the T790M resistance mutation while sparing wild-type EGFR[4,11]. Since its initial accelerated approval for T790M-positive disease in 2015, the clinical development program of osimertinib has expanded markedly, from second-line salvage therapy to first-line metastatic treatment and subsequently to curative-intent perioperative and locally advanced treatment. This trajectory represents one of the most comprehensive and successful targeted therapy development programs in oncology history[12-14]. Over the past decade, an extensive body of literature concerning osimertinib in EGFR-mutated NSCLC has accumulated; however, these contributions tend to be circumscribed by thematic focus or temporal scope[2,12,15-25]. Broad clinical-positioning reviews have typically focused on one or two disease stages, most commonly advanced first-line and T790M-positive later-line settings, without systematically integrating the more recent adjuvant (ADAURA), locally advanced (LAURA), and neoadjuvant (NeoADAURA) evidence into a unified treatment continuum[26-28]. Resistance-focused reviews, while offering valuable molecular depth, have generally cataloged mechanisms in isolation from clinical decision-making algorithms and have rarely provided a structured, line-dependent comparison of on-target vs. off-target resistance patterns across first-line, second-line, and adjuvant contexts[2,12,15,17-24,29]. Meta-analyses and network meta-analyses have quantified systemic efficacy and, in selected cases, central nervous system (CNS)-specific outcomes but have not contextualized these findings within the rapidly shifting frontline landscape now shaped by combination intensification trials such as FLAURA2 and MARIPOSA[30-41]. Similarly, guidelines and consensus documents, although clinically pragmatic, have largely predated the convergence of antibody-drug conjugates, EGFR-MET bispecific antibodies, and fourth-generation allosteric EGFR inhibitors into the postosimertinib therapeutic space[24,42-46]. As a consequence, no single review to date has offered an integrated framework that simultaneously spans the full disease continuum from curative-intent adjuvant therapy through locally advanced consolidation to advanced first-line treatment and mechanism-guided postprogression management. The present review seeks to address this gap by providing, for the first time, a comprehensive and clinically oriented synthesis that unifies six treatment scenarios within a single narrative architecture. It systematically contrasts resistance biology as a function of treatment line and proposes a risk-adapted frontline selection framework informed by the latest biomarker and combination trial evidence. In addition, it maps each identified resistance mechanism to its corresponding therapeutic strategy, with explicit notation of evidence maturity. In doing so, this review also addresses key unresolved questions, including resistance after adjuvant osimertinib, optimal frontline intensity selection, sequencing of novel postosimertinib agents, and the role of minimal residual disease (MRD)-guided adaptive strategies that should inform the design of next-generation clinical trials. By consolidating the most current evidence through early 2026 into a cohesive decision-support framework, this work aims to serve not only as a reference for practicing clinicians navigating an increasingly complex treatment landscape but also as a roadmap for researchers seeking to prioritize the most impactful areas of investigation in EGFR-mutant NSCLC. Osimertinib (AZD9291) is a mono-anilino-pyrimidine compound that functions as an irreversible, covalent inhibitor of EGFR through selective binding to the C797 residue in the adenosine triphosphate (ATP)-binding pocket[4]. Its molecular design strongly inhibits both EGFR-sensitizing mutations (exon 19 deletion, L858R) and the T790M resistance mutation, while it exhibits approximately 200-fold greater selectivity over wild-type EGFR, a property that underpins its favorable therapeutic index compared with earlier-generation TKIs[4,27]. Osimertinib is orally administered at a standard dosage of 80 mg once daily, achieving steady-state plasma concentrations within approximately 15 days, with a terminal half-life of approximately 48 h that supports once-daily dosing. Metabolism occurs primarily via CYP3A4 and CYP3A5, generating two pharmacologically active metabolites (AZ5104 and AZ7550) that contribute to both systemic and intracranial activity[25]. A distinguishing pharmacokinetic feature is the exceptional CNS penetration of osimertinib: preclinical studies have demonstrated a brain-to-plasma area under the concentration–time curve, ratio substantially higher than that of gefitinib, erlotinib, or afatinib, which is attributable to its physicochemical properties, including moderate lipophilicity and low susceptibility to P-glycoprotein-mediated efflux[11]. This pharmacologic profile, mutation-selective potency, wild-type sparing, and CNS penetration provide the mechanistic foundation for the clinical efficacy data reviewed in subsequent sections.
EVIDENCE FROM CLINICAL TRIALS
Overview of the clinical evidence landscape
The prospective interventional evidence base for osimertinib is unusually rich for targeted oncologic agents, encompassing multiple phase III randomized controlled trials and numerous phase II studies across virtually every clinically relevant disease context. Table 1 provides a comprehensive overview of the clinical settings and corresponding key trials.
Clinical settings and key prospective trials of osimertinib
| Clinical setting | Key trials | Phase | Design |
| Adjuvant (post-resection) | ADAURA; OSTAR | III; II | RCT (placebo-controlled); Single-arm |
| Neoadjuvant (preoperative) | NCT03433469; NEOS | II; II | Single-arm; Single-arm |
| Unresectable stage III post-CRT | LAURA | III | RCT (placebo-controlled) |
| First-line metastatic (vs. 1st-gen TKIs) | FLAURA | III | RCT (active-controlled) |
| First-line metastatic (± chemotherapy) | FLAURA2; OPAL | III; II | RCT; Single-arm |
| First-line, special populations | OPEN/TORG2040; LiquidLung-O Cohort 1 | II; II | Single-arm; Single-arm |
| Post-EGFR-TKI, T790M-positive | AURA3; AURA extension; LiquidLung-O Cohort 2; WJOG 8815L; APOLLO; Asia-Pacific; Korean subgroup; Poor PS | III; II | RCT (chemo-controlled); Single-arm studies |
| Uncommon EGFR mutations | KCSG-LU15-09; UNICORN; Pooled post-hoc | II; II | Single-arm; Single-arm |
| Exon 20 insertions | LU17-19 | II | Single-arm |
| Head-to-head vs. 2nd-gen TKI | Heat on beat | II | RCT (active-controlled) |
Curative-intent settings
Adjuvant therapy: The ADAURA program. The ADAURA trial represents a paradigm-shifting contribution to the adjuvant treatment of early-stage EGFR-mutated NSCLC. In this international, double-blind, phase III trial, 682 patients with completely resected stage IB-IIIA NSCLC harboring EGFR ex19del or L858R mutations (1:1) were randomized to receive 80 mg of osimertinib once daily vs. placebo for 3 years[47]. The initial disease-free survival (DFS) analysis demonstrated a dramatic and unprecedented magnitude of benefit: the hazard ratio for DFS was approximately 0.20 in the primary stage II-IIIA population, representing an 80% reduction in the risk of disease recurrence or death[47,48]. Updated analyses confirmed a sustained benefit across all the enrolled stages, with particularly striking CNS DFS protection (hazard ratio [HR] 0.24), underscoring the value of osimertinib in preventing brain relapse, a dominant mode of failure in early-stage disease with EGFR mutations[48,49]. The final overall survival (OS) analysis provided definitive evidence that adjuvant osimertinib is disease-modifying rather than merely delaying recurrence, with a statistically significant and clinically meaningful overall survival advantage in stage II-IIIA patients[50]. This statistically significant and clinically meaningful OS benefit was achieved despite the availability of effective subsequent therapies, including osimertinib at recurrence, which consolidated adjuvant osimertinib as the standard of care for resected stage IB-IIIA EGFR-mutated NSCLC[49]. Given that ADAURA predominantly enrolled stage IB-IIIA patients, the OSTAR trial (phase II, single-arm) extended adjuvant osimertinib into stage I NSCLC with high-risk histologic features (solid/micropapillary pattern ≥ 10%, complex glandular pattern ≥ 15%, or spread through air spaces [STAS])[51]. With 70 patients enrolled and a primary endpoint of 3-year DFS, this study explores the risk-adapted expansion of adjuvant TKI therapy beyond conventional tumor, node, metastasis (TNM) staging[51]. Detailed efficacy data are awaited. A detailed comparison of the ADAURA trials is shown in Supplementary Table 1.
Neoadjuvant osimertinib. Two phase II trials have prospectively evaluated neoadjuvant osimertinib in patients with resectable EGFR-mutated NSCLC. The first trial (NCT03433469) was a multi-institutional study that enrolled 27 patients with stage I–IIIA (AJCC v7) NSCLC harboring EGFR ex19del or L858R mutations, who received up to two 28-day cycles of osimertinib 80 mg daily before surgery. Preliminary results were first reported by Aredo et al. at ASCO 2023, and the full study findings were subsequently published by Blakely et al. in 2024[52,53]. The primary endpoint was major pathologic response (MPR; ≤ 10% viable tumor). Among the 27 treated patients, 24 (89%) underwent successful resection, with acceptable perioperative safety. While radiographic responses were common, MPR rates were modest compared with those of neoadjuvant immunotherapy regimens[52,53]. The second trial, the Neoadjuvant Osimertinib Study (NEOS), was a multicenter, single-arm study in which 6 weeks of neoadjuvant osimertinib was administered to patients with resectable stage II–IIIB EGFR-mutated lung adenocarcinoma[54]. Interim analysis demonstrated favorable radiological responses and high R0 resection rates, supporting the feasibility of this approach[54]. Collectively, these neoadjuvant studies demonstrate that short-term preoperative osimertinib is both feasible and safe, with frequent radiographic tumor shrinkage but more modest pathological responses than those observed with certain neoadjuvant chemoimmunotherapy regimens. However, the incremental contribution of neoadjuvant osimertinib over adjuvant-only strategies remains to be clarified. Detailed information on the neoadjuvant osimertinib trials is provided in Supplementary Table 2.
Unresectable stage III consolidation: The LAURA trial. The LAURA trial addressed a critical unmet need: the management of unresectable stage III EGFR-mutated NSCLC following definitive chemoradiotherapy (CRT). This phase III, double-blind trial randomized 216 patients (2:1) to receive 80 mg osimertinib daily vs. placebo after CRT without progression[55]. The results were striking: the median progression-free survival (PFS) was 39.1 months with osimertinib vs. 5.6 months with placebo, representing one of the greatest PFS gains observed with any consolidation therapy in stage III NSCLC[55]. This magnitude of benefit parallels and arguably exceeds the PFS improvements seen with durvalumab in the PACIFIC trial for unselected stage III NSCLC, although it applies to the molecularly defined EGFR-mutated subset. A critical clinical consideration in LAURA is the careful differentiation between radiation-related and TKI-related pneumonitis, which requires vigilant monitoring and nuanced clinical judgment. The details of the LAURA trial are shown in
First-line advanced/metastatic disease
Osimertinib vs. first-generation EGFR-TKIs: FLAURA The FLAURA trial was a pivotal study that redefined the first-line treatment standard for advanced EGFR-mutated NSCLC. In this phase III trial, 556 treatment-naïve patients with advanced EGFR-ex19del or L858R NSCLC (1:1) were randomized to receive 80 mg osimertinib daily vs. standard-of-care EGFR-TKIs (gefitinib 250 mg or erlotinib 150 mg)[3]. Osimertinib demonstrated a highly significant PFS advantage (HR 0.46), effectively doubling the duration of disease control compared with first-generation TKIs[3,56]. The final OS analysis confirmed a statistically significant survival advantage despite substantial crossover from the control arm, with postprogression analyses indicating that the observed benefit was conservative given the high crossover rate[56,57]. Notably, FLAURA also reduced CNS progression and improved intracranial disease control when it was combined with osimertinib, which is consistent with its superior ability to penetrate the blood-brain barrier[58]. The safety and tolerability advantages of osimertinib over first-generation TKIs observed in FLAURA are discussed in Section "COMPREHENSIVE SAFETY ASSESSMENT". The detailed trial data of FLAURA are summarized in Supplementary Table 4.
Osimertinib plus chemotherapy. Since the FLAURA trial established osimertinib monotherapy as the first-line standard for EGFR-mutated advanced NSCLC, attention has turned to whether combining osimertinib with platinum-based chemotherapy could further improve outcomes by delaying or overcoming resistance. This question has been prospectively addressed by two key trials: FLAURA2 and OPAL. FLAURA2 is a phase III, open-label trial in which 557 treatment-naïve patients with advanced EGFR ex19del or L858R NSCLC were randomized to osimertinib plus platinum-pemetrexed (4 induction cycles followed by osimertinib-pemetrexed maintenance) vs. osimertinib monotherapy[59,60]. Studies have reported that PFS is significantly longer with the combination than with monotherapy[59]. A final OS analysis has been performed[60], and whether the improvement in PFS translates to a definitive survival advantage, a critical determinant for broad adoption of this intensification strategy, has been determined. OPAL is a phase II, multicenter study that evaluated the combination of osimertinib with cisplatin or carboplatin plus pemetrexed in 67 previously untreated patients, confirming the feasibility, high response rates, and expected chemotherapy-related toxicity of the regimen[61]. The detailed trial data of FLAURA 2 and OPAL are summarized in Supplementary Table 5.
First-line osimertinib in special populations. More trials have been performed in certain populations; for poor performance status (OPEN/TORG2040), patients with Eastern Cooperative Oncology Group performance status (ECOG PS) of 2–4 have been historically underrepresented in pivotal TKI trials. The OPEN/TORG2040 multicenter phase II trial enrolled 30 previously untreated advanced EGFR-mutated patients (22 PS 2, 6 PS 3, 2 PS 4; median age 75 years) to receive first-line osimertinib[62,63]. The trial reported both tumor responses and PS improvement in this elderly, frail cohort with manageable toxicity, supporting osimertinib as a viable and likely preferable option to chemotherapy or older TKIs for poor-PS patients[62,63]. Another trial assessed a circulating tumor DNA (ctDNA)-selected first-line (LiquidLung-O Cohort 1) population. In this phase II trial, patients were enrolled on the basis of ctDNA-detected activating EGFR mutations[16]. In the ex19del subgroup (n = 11), the objective response rate (ORR) was 91%, with a median PFS of 21.9 months (95% confidence interval [CI]: 5.5-38.3); in the L858R/L861Q subgroup, the ORR was 43%, with a median PFS of only 5.1 months (95%CI: 2.3-7.9)[64]. Despite an extremely high baseline CNS metastasis incidence (~79%), the long PFS in ex19del patients was notable. This study confirmed the feasibility of ctDNA-based treatment selection and strongly illustrated the mutation-specific heterogeneity of benefit.
Second line and beyond
Randomized evidence: The AURA3 phase III trial randomized patients (2:1) with T790M-positive advanced NSCLC after progression on first/second-generation EGFR-TKIs to 80 mg of osimertinib daily vs. platinum-pemetrexed[65]. Osimertinib demonstrated superior PFS across all the subgroups, with a particularly pronounced benefit in the Japanese subgroup (HR 0.27)[66]. Detailed efficacy and safety comparisons from the AURA3 trial are presented in Supplementary Table 6.
Phase II and regional cohort studies. More phase II and regional cohort studies have reinforced the AURA3 findings, providing complementary evidence across diverse populations and biopsy modalities. Across these studies, osimertinib consistently yields an ORR of approximately 65%-75% and a median PFS of 8-13 months in T790M-positive patients[67-69]. Its activity is maintained in plasma-only T790M and CNS-metastatic subsets, although PFS is somewhat attenuated in plasma-selected (8.3 months[68]) vs. tissue-confirmed (12 months[67]) cohorts, likely reflecting differences in disease burden and molecular heterogeneity. These trials are summarized in Supplementary Table 7.
Mutation-specific considerations
Common sensitizing mutations: exon 19 deletion vs. L858R. In first-line and ctDNA-selected trials, ex19del is consistently associated with superior outcomes compared with L858R. The Liquid Lung-O Cohort 1 data illustrate the following: an ex19del ORR of 91%, with a median PFS of 21.9 months, vs. an L858R/L861Q ORR of 43%, with a median PFS of 5.1 months[64]. Similar differential patterns are observed across FLAURA and other datasets, reflecting intrinsic biological differences between these mutation subtypes.
Uncommon EGFR mutations (excluding exon 20 insertions). Three prospective studies reported osimertinib activity in patients with uncommon EGFR mutations. The KCSG-LU15-09 phase II trial (Korean Cancer Study Group; NCT03001505) demonstrated clinically meaningful activity, with an ORR of 50% and a median PFS of 8.2 months[70], whereas the UNICORN trial extended this evidence to the first-line, untreated setting with meaningful responses[71,72]. A pooled post hoc analysis by Eide et al. revealed an important mutation-specific gradient: compared with other uncommon variants, G719X-compound mutations markedly improved outcomes, suggesting that mutation subtypes should guide clinical expectations and treatment counseling[73]. These data collectively support the use of osimertinib for several key uncommon genotypes, particularly G719X, L861Q, and S768I. Supplementary Table 8 summarizes osimertinib in patients with uncommon EGFR mutations.
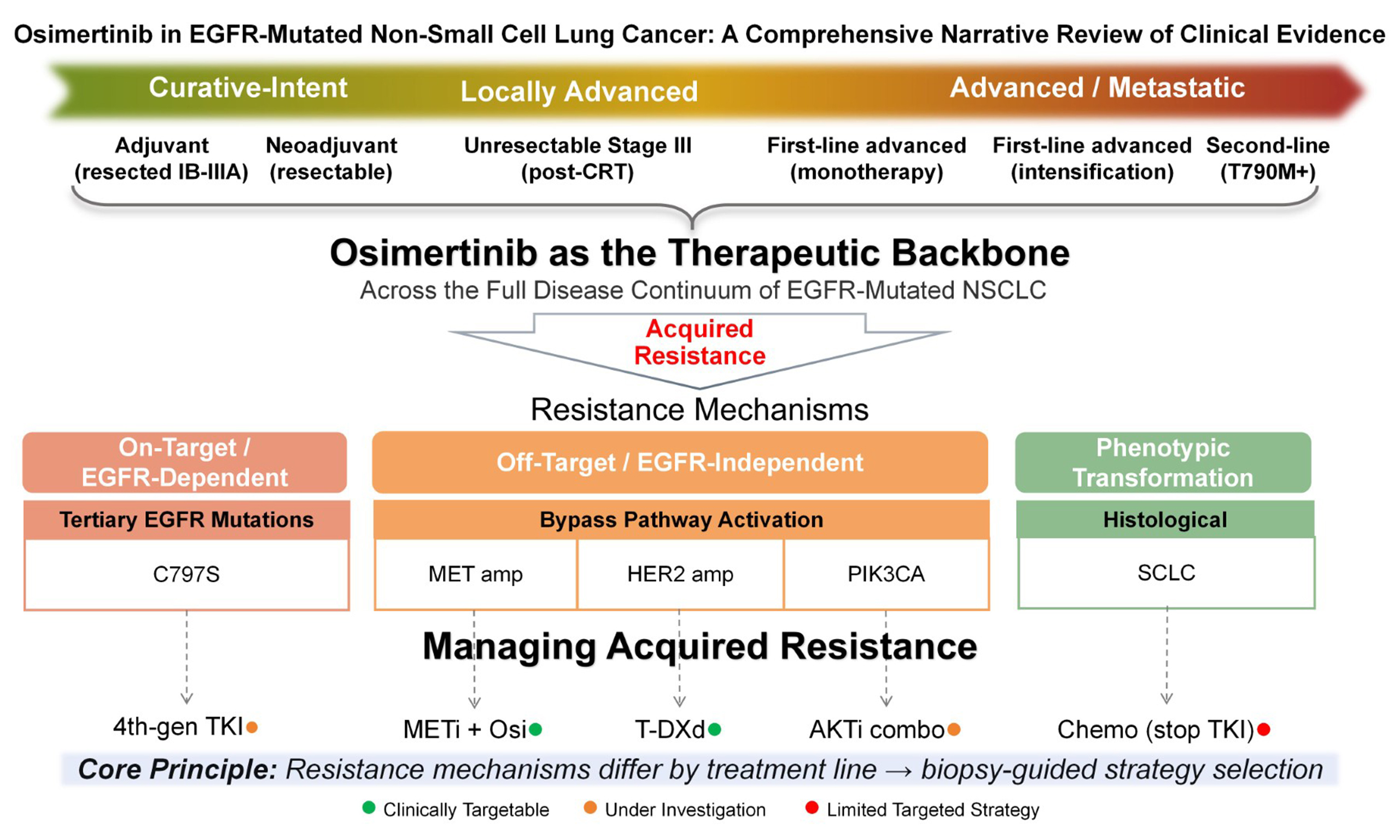
Exon 20 insertions: the Korean LU17-19 phase II trial evaluated 80 mg osimertinib daily in patients with EGFR exon 20 insertion mutations after chemotherapy failure[74]. Consistent with preclinical data suggesting structural resistance at standard dosing, the available evidence indicates limited activity. Standard-dose osimertinib is not an optimal therapy for most exon 20 insertions, reinforcing the need for exon 20-specific agents (e.g., amivantamab and mobocertinib) and demonstrating the boundaries of the mutation spectrum of osimertinib. The resistance mechanisms of osimertinib in lung cancer are summarized in Figure 1. Importantly, these resistance mechanisms differ substantially in their current therapeutic actionability and should be interpreted along a translational readiness spectrum rather than as a homogeneous catalog. Among the clinically targetable mechanisms with established or late-phase therapeutic options, MET amplification can be addressed with selective MET inhibitors (savolitinib, tepotinib, and capmatinib) or the EGFR-MET bispecific antibody amivantamab, all of which have generated confirmatory clinical efficacy data in osimertinib-resistant populations; Human epidermal growth factor receptor 2 (HER2) amplification is targeted by trastuzumab deruxtecan (T-DXd), which has demonstrated meaningful activity across HER2-altered NSCLC; oncogene fusions involving anaplastic lymphoma kinase (ALK), rearranged during transfection (RET), ROS proto-oncogene 1 (ROS1), or neurotrophic tyrosine receptor kinase (NTRK) can be managed with the corresponding approved selective TKI (e.g., alectinib/lorlatinib for ALK and selpercatinib for RET), provided that the fusion is identified through comprehensive genomic profiling at progression. Among the mechanisms currently under active clinical investigation but not yet supported by definitive practice-changing evidence, the tertiary C797S mutation in EGFR exon 20, which disrupts the covalent binding site of osimertinib, is being targeted by fourth-generation allosteric EGFR inhibitors (e.g., BLU-945 and BLU-525) in early-phase trials with preliminary signals of activity; PIK3CA (phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha) mutations and PTEN (phosphatase and tensin homolog) loss are being explored as targets for AKT (protein kinase B) inhibitors (e.g., capivasertib) in combination strategies, and RAS/MAPK (rat sarcoma viral oncogene homolog/mitogen-activated protein kinase) pathway activation is under investigation with MEK inhibitor combinations, although clinical data remain limited. Among the mechanisms for which no targeted therapeutic strategy is currently established, histological transformation to small-cell lung cancer (SCLC), The prevalence of SCLC transformation (2%–15%) and its management with platinum–etoposide chemotherapy remain accurately described. The parallel statement on squamous cell transformation correctly reflects the absence of a mechanism-specific therapeutic strategy. The discussion of rare or polyclonal resistance profiles preserves the original meaning regarding the limitations of current single-target approaches. This stratification of resistance mechanisms by therapeutic actionability has direct clinical implications: it underscores the critical importance of comprehensive molecular profiling at the time of osimertinib progression, ideally through both tissue rebiopsy and liquid biopsy, to distinguish patients who can be redirected to established targeted strategies from those for whom clinical trial enrollment or empirical chemotherapy-based approaches remain more appropriate.
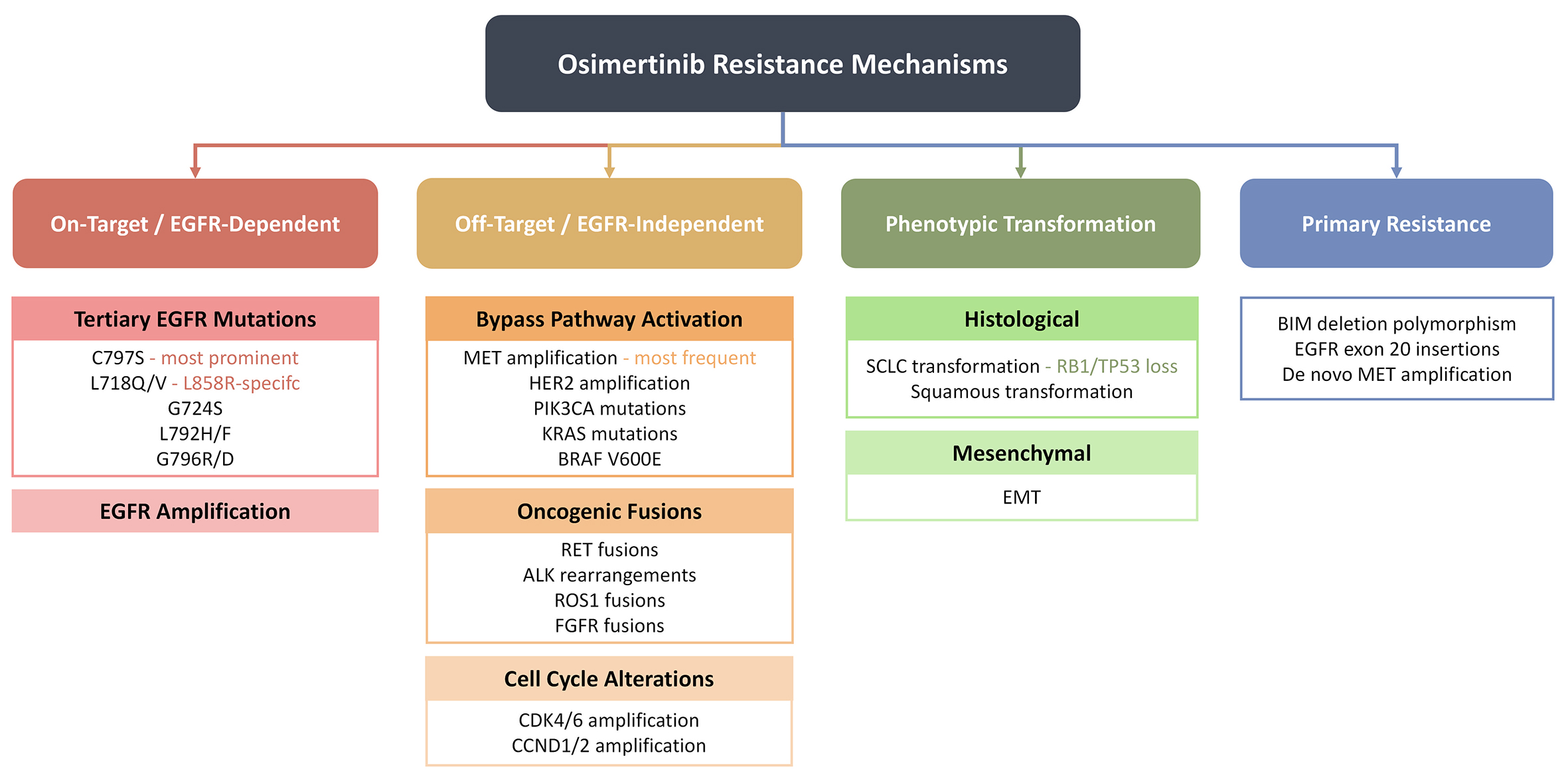
Figure 1. Mechanisms of osimertinib resistance. Note: Resistance mechanisms are classified by current therapeutic actionability. Clinically targetable: MET amplification (savolitinib, tepotinib, and amivantamab), HER2 amplification (trastuzumab deruxtecan), and ALK/RET/ROS1/NTRK fusions (corresponding selective TKIs). Under clinical investigation: C797S mutation (fourth-generation allosteric EGFR inhibitors, e.g., BLU-945), PIK3CA/PTEN alterations (AKT inhibitors), and RAS/MAPK activation (MEK inhibitor combinations). No established targeted strategy exists for SCLC: histological transformation (managed with platinum-etoposide chemotherapy), squamous transformation, or polyclonal multipathway resistance.
EFFICACY OF THE CENTRAL NERVOUS SYSTEM
CNS metastases represent a dominant mode of treatment failure and a leading cause of morbidity in patients with EGFR-mutated NSCLC, with brain involvement occurring in approximately one-third of patients during the course of their disease and having a disproportionate effect on functional independence and quality of life[75]. The limited CNS penetration of first- and second-generation EGFR-TKIs has been a longstanding therapeutic liability, as the blood-brain barrier restricts intracranial drug concentrations to subtherapeutic levels, permitting the CNS to serve as a pharmacologic sanctuary for residual disease even when systemic control is maintained[11]. Osimertinib was rationally designed to overcome this limitation: preclinical studies demonstrated sustained brain exposure and antitumor activity in multiple EGFR-mutant NSCLC brain metastasis models, with substantially greater CNS penetration than gefitinib, erlotinib, and afatinib did, establishing the pharmacokinetic basis for its subsequent clinical CNS efficacy[11]. This preclinical advantage has been validated across a remarkably broad spectrum of prospective clinical trials, evolving from early exploratory subanalyses to formal, protocol-specified end points that now constitute a central element of osimertinib’s therapeutic identity.
The first comparative clinical evidence for osimertinib’s intracranial activity emerged from the T790M-positive second-line setting. Preplanned CNS analysis of the AURA3 phase III trial evaluated osimertinib vs. platinum pemetrexed in patients with T790M-positive advanced NSCLC whose baseline brain metastases were confirmed by a blinded central neuroradiologic review[76]. In this CNS-evaluable population, compared with chemotherapy, osimertinib resulted in significantly higher intracranial objective response rates and prolonged CNS progression-free survival. These findings were particularly impactful because they provided the first randomized evidence that a TKI could achieve not only systemic disease control but also measurable and durable intracranial tumor shrinkage in a head-to-head comparison with platinum-based chemotherapy, a treatment modality with inherently poor CNS penetration. The APOLLO study extended this evidence to a more clinically representative population: prospectively enrolling T790M-positive NSCLC patients with documented CNS metastases, the trial confirmed meaningful systemic and intracranial PFS with 80 mg of osimertinib daily[77]. Uniquely among osimertinib trials, APOLLO integrated cerebrospinal fluid (CSF) pharmacokinetic measurements and next-generation sequencing analyses, providing direct evidence of osimertinib penetration into the CSF compartment and enabling molecular characterization of intracranial vs. extracranial disease evolution. This translational integration reinforced the mechanistic rationale for osimertinib’s CNS efficacy and offered insights into patterns of intracranial resistance that remain relevant to ongoing drug development efforts. Korean subgroup analysis of the AURA extension and AURA2 trials further confirmed this CNS activity in an East Asian population, with trial protocols explicitly permitting the enrollment of patients with stable or asymptomatic brain metastases, a design feature that enhanced the generalizability of the CNS efficacy signal beyond the narrowly selected populations typical of earlier targeted therapy studies[69].
The transition of osimertinib to first-line metastatic therapy in the FLAURA trial brought CNS outcomes into even sharper focus. FLAURA enrolled patients with asymptomatic or stable CNS metastases and demonstrated that compared with standard-of-care first-generation EGFR-TKIs (gefitinib or erlotinib), osimertinib significantly reduced the risk of CNS progression[3,56]. A dedicated CNS subgroup analysis from FLAURA reported superior CNS response rates and CNS PFS with osimertinib vs. the comparator arm in patients with identifiable brain lesions at baseline[58]. Moreover, among patients without baseline CNS metastases, osimertinib reduced the incidence of new brain lesions during treatment, a preventive benefit that extends the CNS efficacy narrative beyond the treatment of established metastases to prospective CNS protection. This dual capacity, both therapeutic intracranial activity against existing lesions and prophylactic prevention of new CNS disease, distinguishes osimertinib from its predecessors and has become a decisive factor in clinical decision-making, particularly for patients with a high a priori risk of CNS relapse. The ctDNA-selected Liquid Lung-O Cohort 1 trial provides a striking illustration of this principle: Despite an extraordinarily high baseline incidence of CNS metastases (79%), patients with exon 19 deletion who were treated with first-line osimertinib achieved an ORR of 91% and a median PFS of 21.9 months[64]. That such prolonged disease control was achievable in a cohort with near-universal intracranial involvement testifies to the magnitude of osimertinib’s CNS activity in the first-line setting and underscores its preferential value in patients presenting with brain disease at diagnosis.
The extension of osimertinib into curative-intent settings, adjuvant and postchemoradiation consolidation, has increased CNS disease control from a secondary consideration to a primary rationale for therapy. In the ADAURA trial, CNS DFS was incorporated as a protocol-specified secondary endpoint, reflecting the recognition that CNS relapse is a particularly devastating event in patients who have undergone curative resection[48]. The results were unequivocal: the CNS DFS hazard ratio was 0.24 in the stage II-IIIA population, indicating a 76% reduction in the risk of CNS recurrence with adjuvant osimertinib compared with placebo. This magnitude of CNS protection is arguably the single most clinically persuasive argument for adjuvant osimertinib in resected EGFR-mutated NSCLC, given that isolated CNS relapse following complete surgical resection often signals the transition from curable to incurable disease and disproportionately compromises neurologic function and patient autonomy. Updated analyses with longer follow-up confirmed the sustained durability of this CNS DFS benefit, further reinforcing its relevance to long-term survival. In the locally advanced, unresectable setting, the LAURA trial similarly demonstrated a profound PFS benefit (39.1 vs. 5.6 months with placebo) following definitive CRT[55]. While the trial’s abstract-level reporting does not provide a separate CNS PFS analysis, the extreme prolongation of overall PFS, which is more than sevenfold that of the placebo, necessarily incorporates a substantial component of CNS relapse prevention, given the high baseline risk of brain involvement in stage III EGFR-mutated disease and the known propensity for CNS failure following chemoradiation alone.
Taken together, the evidence of the efficacy of the CNS across the clinical development program of osimertinib reveals a coherent and compelling narrative that has itself undergone a significant methodologic evolution. In the earliest trials (AURA extension, AURA3), CNS outcomes were assessed through preplanned but exploratory subgroup analyses. As the clinical significance of intracranial disease control became evident, subsequent trials progressively formalized CNS endpoints: FLAURA incorporated CNS progression as a component of the primary PFS analysis and conducted dedicated CNS subgroup evaluations; ADAURA elevated CNS DFS to a protocol-specified secondary endpoint with structured neuroradiologic review; and the APOLLO study uniquely integrated CSF-based pharmacokinetic and genomic correlates. This methodologic maturation, from retrospective observation to prospective, protocol-mandated CNS assessment, reflects both the growing recognition of CNS relapse as a critical determinant of long-term outcomes in EGFR-mutated NSCLC and the field’s increasing confidence in osimertinib’s ability to address this challenge.
The clinical implications of this CNS evidence base are substantial and multidimensional. For patients who present with brain metastases at any stage of EGFR-mutated NSCLC, the advantages of osimertinib over both chemotherapy and first-generation TKIs in terms of intracranial ORR and CNS PFS suggest that osimertinib is the pharmacologic agent of first choice, with the potential to modify the need for, timing of, or extent of local CNS therapies such as stereotactic radiosurgery or whole-brain radiation. For patients without baseline CNS disease, the demonstrated reduction in new brain lesion development and the dramatic improvement in CNS DFS in the adjuvant setting (HR 0.24) provide a strong pharmacologic rationale for osimertinib as a CNS-protective strategy. With respect to the growing population of long-term osimertinib responders in adjuvant and consolidation settings, the prevention of CNS relapse translates directly into the preservation of neurocognitive function, functional independence, and quality of life outcomes, which are not captured in traditional PFS or OS endpoints but are of paramount importance to patients and are increasingly recognized by regulatory and guideline bodies. Taken together, the CNS activity of osimertinib is not merely an ancillary benefit appended to its systemic efficacy; it is a therapeutically decisive and pharmacologically distinctive property that pervades every clinical setting in which the drug has been evaluated and constitutes one of the strongest arguments for its position as the backbone EGFR-targeted agent across the full NSCLC disease continuum. Table 2 provides key evidence of the CNS efficacy of osimertinib.
CNS efficacy of osimertinib across clinical settings: summary of key evidence
| Clinical setting | Study | Population | Comparator | CNS endpoint (s) | Key CNS efficacy findings | Unique methodologic features | Clinical implications |
| Preclinical | Ballard et al.[11] | EGFR-mutant NSCLC brain metastases models | Gefitinib, erlotinib, afatinib | Brain exposure; intracranial tumor growth inhibition | Substantially greater CNS penetration and sustained brain exposure vs all comparator EGFR-TKIs | Multiple in vivo brain metastases models; steady-state brain-to-plasma ratio quantification | Established the pharmacokinetic rationale for osimertinib's clinical CNS activity; informed all subsequent CNS-focused trial designs |
| T790M+ post-EGFR-TKI (Phase III) | AURA3 CNS analysis[76] | T790M-positive advanced NSCLC with baseline brain metastases (blinded central neuroradiologic review) | Platinum-pemetrexed | CNS ORR (primary CNS endpoint); CNS PFS; CNS DoR | Significantly higher CNS ORR and longer CNS PFS with osimertinib vs chemotherapy | First randomized comparative CNS efficacy evidence for any EGFR-TKI; blinded independent central neuroradiologic review | Established osimertinib as superior to chemotherapy for measurable intracranial disease in T790M+ patients; influenced subsequent CNS endpoint design |
| T790M+ post-EGFR-TKI (Phase III, Japan) | AURA3 Japanese subgroup[66] | Japanese T790M+ patients (n = 41 osi, n = 22 chemo); stable/asymptomatic brain metastases permitted | Platinum-pemetrexed | PFS (includes CNS events) | Median PFS 12.5 vs. 4.3 months; HR 0.27 (95%CI: 0.13-0.56) | Japanese-specific subgroup; consistent with global CNS benefit | Confirmed CNS-inclusive PFS advantage in East Asian population |
| T790M+ with CNS metastases (Phase II) | APOLLO[77] | T790M-positive NSCLC with documented CNS metastases | None (single-arm) | Overall PFS (PFS-o); ORR; AEs | Meaningful systemic and intracranial PFS demonstrated | CSF pharmacokinetic measurements confirming drug penetration; CSF next-generation sequencing characterizing intracranial molecular evolution | Direct evidence of osimertinib CSF penetration; molecular insights into intracranial vs. extracranial resistance patterns |
| T790M+, Korean subgroup (Phase II) | Korean AURA ext/AURA2[69] | Korean T790M+ patients (n = 66 treated, 62 evaluable); stable/asymptomatic brain metastases permitted | None (single-arm subgroup) | ORR; DoR | ORR 74%; median DoR 9.8 months | Explicit inclusion of patients with stable brain metastases; East Asian population confirmation | Generalizability of CNS benefit to East Asian populations with baseline brain involvement |
| 1st-line metastatic (Phase III) | FLAURA CNS analysis[58] | Treatment-naïve advanced EGFR ex19del/L858R; asymptomatic/stable CNS metastases included (N = 556) | Gefitinib/erlotinib | CNS ORR; CNS PFS; new CNS lesion incidence | Superior CNS ORR and CNS PFS vs. first-generation TKIs; reduced incidence of new brain lesions in patients without baseline CNS disease[1,2,149] | Preplanned CNS subgroup analysis; CNS progression included in primary PFS composite; brain scans not mandated but performed when clinically indicated | Dual benefit: therapeutic (shrinkage of existing lesions) and prophylactic (prevention of new CNS metastases); key differentiator from 1st-gen TKIs |
| 1st-line, ctDNA-selected (Phase II) | LiquidLung-O Cohort 1[64] | Untreated EGFR-mut, ctDNA-positive (n = 19); baseline CNS metastasis prevalence ~79% | None (single-arm) | ORR; PFS (systemic, CNS-inclusive) | Ex19del: ORR 91%, median PFS 21.9 months despite near-universal (~79%) baseline CNS involvement; L858R/L861Q: ORR 43%, PFS 5.1 months | Extremely high baseline brain metastasis prevalence (~79%); ctDNA-based patient selection | Demonstrates prolonged disease control achievable even with near-universal CNS involvement; strongest illustration of mutation-specific CNS benefit (ex19del >> L858R) |
| Adjuvant (Phase III) | ADAURA CNS DFS[48,49] | Completely resected stage IB-IIIA EGFR ex19del/L858R (N = 682) | Placebo | CNS DFS (protocol-specified secondary endpoint) | CNS DFS HR 0.24 in stage II-IIIA (76% risk reduction in CNS recurrence vs. placebo); sustained with longer follow-up | First adjuvant trial with CNS DFS as a formal, protocol-specified endpoint; structured neuroradiologic review | Arguably the most clinically consequential CNS finding: prevention of isolated CNS relapse preserves curability, neurocognitive function, and patient autonomy after complete resection |
| Post-CRT consolidation (Phase III) | LAURA[55] | Unresectable stage III EGFR-mutated post-CRT (N = 216; 143 osi, 73 placebo) | Placebo | PFS (CNS-inclusive); separate CNS analysis not in excerpt | Median PFS 39.1 vs. 5.6 months (> 7-fold prolongation); necessarily incorporates substantial CNS relapse prevention given high baseline CNS risk in stage III | Post-chemoradiotherapy context; high a priori CNS relapse risk; competing pneumonitis risks | Extreme PFS prolongation includes a major CNS-protective component; extends the CNS benefit paradigm from metastatic/adjuvant into locally advanced unresectable disease |
COMPREHENSIVE SAFETY ASSESSMENT
Building on the efficacy data presented in Section "EVIDENCE FROM CLINICAL TRIALS", this section provides a consolidated, cross-sectional analysis of the safety profile of osimertinib. To avoid fragmented presentation of safety data across individual trial descriptions, all tolerability and adverse event information has been centralized here to facilitate meaningful cross-trial comparisons.
The safety evaluation of osimertinib benefits from an unusually consistent pharmacologic framework: across virtually all prospective interventional trials reviewed, spanning adjuvant, neoadjuvant, consolidation, first-line, and salvage settings, the drug has been administered at a uniform dosage of 80 mg once daily[52,53,66,69,70,73]. This dosing consistency facilitates meaningful cross-trial safety comparisons and enables a cumulative, setting-stratified characterization of the tolerability profile that is rarely achievable for targeted oncologic agents. Table 3 summarizes the key adverse event profiles of osimertinib across all major clinical settings.
Safety profile of osimertinib across clinical settings: summary of key adverse event data
| Clinical setting | Study | Population | Common AEs (any grade) | Serious/Notable AEs | Grade ≥ 3 AEs | Discontinuation/Fatal events | Key safety considerations |
| T790M+ post-EGFR-TKI (Phase II) | AURA Extension[67] | Pretreated T790M+ advanced NSCLC | Diarrhea 43%; Rash 40%; Paronychia, dry skin, decreased appetite (variably reported) | ILD/pneumonitis ~4% | Not separately reported in excerpt | 3 fatal (grade 5) ILD events | Most granular single-trial safety dataset; ILD fatality rate underscores need for vigilance |
| T790M+ post-EGFR-TKI (Phase III, Japan) | AURA3 Japanese subgroup[66] | Japanese T790M+ post-TKI (n = 41 osi, n = 22 chemo) | Not individually itemized in excerpt | ILD/pneumonitis reported | Grade ≥ 3 TRAEs: 12.2% (osi) vs. 54.5% (chemo) | - | Dramatically lower high-grade toxicity vs. platinum-pemetrexed; East Asian ILD risk noted |
| T790M+ post-EGFR-TKI (Phase III, global) | AURA3[76] | T790M+ advanced NSCLC (N = 419) | Better tolerated than chemotherapy overall | ILD/pneumonitis reported | Lower than chemotherapy arm | - | Osimertinib better tolerated than platinum-pemetrexed across endpoints |
| T790M+, plasma-selected (2nd-line) | LiquidLung-O Cohort 2[68] | Plasma T790M+ (n = 19 treated, 15 evaluable) | AEs in 89.5% of patients | 1 grade 3 interstitial pneumonitis | Grade 3-4 AEs: 31.6% | 1 discontinuation for ILD | Plasma-selected cohorts may include more heavily pretreated patients with higher AE burden |
| T790M+, CNS metastases | APOLLO[77] | T790M+ with CNS metastases | AEs reported; details in source | CSF PK and NGS analyses performed | - | - | Unique integration of CSF pharmacokinetics with safety assessment |
| T790M+, Korean subgroup | Korean AURA ext/AURA2[69] | Korean T790M+ (n = 66 treated) | Consistent with global AURA profile | - | Consistent with global AURA | - | Confirms safety consistency in East Asian population |
| T790M+, real-world (global) | ASTRIS[78] | > 3,000 T790M+ patients, post-EGFR-TKI | Consistent with trial data | ILD/pneumonitis ~1% | - | - | Lower real-world ILD rate vs. clinical trials; may reflect reporting differences |
| T790M+, real-world (Korea) | Korean multicenter[79] | 558 T790M+ patients | Consistent with trial data | Pneumonitis reported | - | Severe AE discontinuation: 1.8% | Real-world confirmation of manageable toxicity across heterogeneous practice |
| T790M+, real-world (Taiwan) | Taiwanese EAP[81] | 419 heavily pretreated patients (53% ≥ 3 prior lines) | Consistent with trial data | - | - | - | Safety maintained in heavily pretreated, real-world population |
| 1st-line metastatic (Phase III) | FLAURA[56] | Treatment-naïve advanced EGFR ex19del/L858R (N = 556) | Lower high-grade rash and diarrhea vs. gefitinib/erlotinib | - | Lower rate vs. 1st-gen TKIs | - | Superior tolerability profile was key driver of first-line adoption |
| 1st-line metastatic + chemo (Phase III) | FLAURA2[59-60] | Treatment-naïve advanced EGFR ex19del/L858R (N = 557) | Additive chemo toxicities: myelosuppression, nausea, fatigue | - | Higher than monotherapy (expected) | - | Incremental chemo toxicity must be weighed against PFS gain |
| 1st-line metastatic + chemo (Phase II) | OPAL[61] | Treatment-naïve EGFR-mutated advanced NSCLC (N = 67) | Expected chemo-related toxicities | Safety was co-primary endpoint | - | - | Confirms feasibility and manageability of combination regimen |
| 1st-line, ctDNA-selected | LiquidLung-O Cohort 1[64] | Untreated EGFR-mut, ctDNA+ (n = 19) | - | 1 drug-related interstitial pneumonitis | - | 1 discontinuation for ILD | Small sample; notable for high CNS metastasis prevalence (~79%) |
| 1st-line, poor PS (PS 2-4) | OPEN/TORG2040[62] | Untreated EGFR-mut, PS 2-4 (n = 30; median age 75 yr) | Formally evaluated; tolerable | - | - | - | Tolerable in elderly/frail; PS improvement observed under treatment |
| Uncommon EGFR mutations | KCSG-LU15-09[70] | Uncommon EGFR mut (n = 36 evaluable) | Rash 31%; Pruritus 25%; Decreased appetite 25%; Diarrhea 22%; Dyspnea 22% | All manageable | - | - | Slightly lower common-AE rates than in classical-mutation trials |
| Adjuvant (3-year dosing) | ADAURA[47,48] | Resected IB-IIIA EGFR-mut (n = 339 osi) | Generally well tolerated | ILD, QTc prolongation, cardiomyopathy monitored | - | - | Prolonged 3-year exposure; structured cardiac monitoring; no major new signals at final OS analysis |
| Neoadjuvant (short-course) | Blakely/Aredo[52] | Resectable I-IIIA EGFR-mut (n = 27) | Median 56 days exposure pre-surgery | No major perioperative complications | - | - | 89% successful resection; no wound healing impairment |
| Neoadjuvant (short-course) | NEOS[54] | Resectable II-IIIB EGFR-mut | 6 weeks exposure pre-surgery | Feasible; no major safety signals | - | - | High R0 resection rate; short exposure minimizes perioperative risk |
| Post-CRT consolidation | LAURA[55] | Unresectable stage III EGFR-mut, post-CRT (n = 143 osi) | - | Competing risk: radiation pneumonitis vs. TKI-related ILD | - | - | Most critical safety context; requires careful pneumonitis attribution; heightened monitoring essential |
The most frequently reported adverse events are dermatologic and gastrointestinal in nature, reflecting on-target EGFR inhibition in epithelial tissues. In the AURA phase II extension cohort, which provides among the most granular safety data in the pretreated T790M-positive population, diarrhea occurred in 43% and rash in 40% of patients, predominantly at grades 1-2[67]. The KCSG-LU15-09 trial in uncommon EGFR mutations reported a broadly similar but somewhat attenuated toxicity spectrum: rash 31%, pruritus 25%, decreased appetite 25%, diarrhea 22%, and dyspnea 22%, all at manageable grades[70]. A defining feature of osimertinib tolerability, which is consistently observed across settings, is the lower incidence and reduced severity of these class-effect toxicities relative to first- and second-generation EGFR-TKIs. In FLAURA, compared with gefitinib/erlotinib, osimertinib resulted in notably fewer high-grade rash and diarrhea events[3,56], while the AURA3 Japanese subgroup analysis strongly revealed this advantage: grade ≥ 3 treatment-related adverse events occurred in only 12.2% of osimertinib-treated patients vs. 54.5% of those receiving platinum pemetrexed[66]. This favorable therapeutic index, lower toxicity burden coupled with superior efficacy, was instrumental in the rapid adoption of osimertinib as the preferred EGFR-TKI across treatment lines.
In light of this background of generally mild and predictable toxicity, interstitial lung disease (ILD) and pneumonitis have emerged as the most clinically consequential idiosyncratic risks, warranting particular vigilance. In the AURA phase II extension, ILD events were documented in approximately 4% of patients, including three fatal (grade 5) cases, indicating that even with a highly selective third-generation TKI, pulmonary toxicity remains a life-threatening concern[67]. In the Liquid Lung-O program, both Cohort 1 (first-line ctDNA-selected) and Cohort 2 (second-line plasma T790M-positive) reported sporadic drug-related interstitial pneumonitis events leading to treatment discontinuation: one patient in Cohort 1[64] and one grade 3 event among 19 treated patients in Cohort 2 (an overall adverse event rate of 89.5% and a grade 3 to 4 rate of 31.6%)[68]. Large-scale real-world data provide a complementary perspective: a global ASTRIS study of > 3,000 T790M-positive patients reported ILD/pneumonitis in approximately 1% of the overall cohort[78], whereas a Korean multicenter real-world study reported treatment discontinuation due to severe adverse events (including pneumonitis) in 1.8% of 558 patients[79]. The apparent discrepancy between clinical trial ILD rates (approximately 4% in AURA extension[67]) and real-world estimates (1%-2%) may reflect differences in reporting rigor, surveillance intensity, population selection, and the inherent difficulty of attributing pulmonary events in heavily pretreated patients with underlying lung disease.
The risk of ILD has particular clinical significance in the postchemoradiotherapy consolidation setting. In LAURA, the overlapping pathophysiology of radiation pneumonitis and TKI-related ILD creates a uniquely challenging diagnostic and management environment[55]. Careful separation of radiotherapy-induced vs. drug-induced pulmonary toxicity is essential for appropriate clinical decision-making, including treatment continuation, dose modification, or discontinuation. Although LAURA’s abstract-level reporting does not provide granular ILD or pneumonitis incidence data, this competing risk is explicitly recognized as central to the benefit risk calculus of post-CRT osimertinib consolidation. Clinicians who prescribe osimertinib in this context must maintain heightened surveillance, particularly during the first months of therapy, when the temporal overlap between radiation-induced and TKI-induced pneumonitis is greatest. East Asian populations deserve additional consideration, as background ILD risk may be elevated in this demographic, a pattern observed across multiple EGFR-TKI classes[66,67].
Cardiac toxicity represents a second domain of structured monitoring throughout the osimertinib program. Corrected QT interval (QTc) prolongation and a reduction in the left ventricular ejection fraction (LVEF) were prospectively assessed in the ADAURA adjuvant trial and its long-term extensions, with cardiac imaging and electrocardiographic surveillance incorporated into the study protocols[47,48,50]. Reassuringly, no major new cardiac safety signals have emerged from these prolonged follow-up analyses, even with 3-year continuous dosing in the adjuvant context. Nevertheless, the cumulative cardiac exposure inherent in extended adjuvant therapy mandates ongoing monitoring, particularly in older patients and those with preexisting cardiovascular comorbidities. The absence of a dedicated cardiac-focused analysis across the combined prospective database remains a relative gap, and long-term postmarketing registries will be essential for definitively characterizing the incidence and clinical significance of osimertinib-associated cardiotoxicity over multiple years of exposure.
The safety profile of osimertinib is further modulated by the specific clinical context in which it is deployed. In perioperative settings, short-term neoadjuvant exposure (6 to 8 weeks) in the Blakely or Aredo trial and NEOS yielded high surgical feasibility, and resection was successfully performed in 89% of patients in NCT03433469, with no sign of impaired wound healing or elevated perioperative morbidity[52-54]. This finding contrasts with the more prolonged perioperative toxicity profiles observed with some chemoimmunotherapy regimens and supports the safety of brief preoperative osimertinib courses. When osimertinib is combined with platinum-pemetrexed chemotherapy, as evaluated in FLAURA2 and OPAL, the predictable additive burden of chemotherapy-related toxicity, principally myelosuppression, nausea, vomiting, and fatigue, is layered onto the baseline profile of the TKI[60]. The FLAURA2 and OPAL trial designs included safety as a coprimary or key secondary endpoint, and the combination was deemed manageable in both studies[59-61], although the incremental toxicity cost relative to monotherapy must be weighed against the PFS benefit, particularly in patients for whom quality of life is a primary treatment goal. In special populations historically excluded from pivotal trials, the OPEN/TORG2040 experience in ECOG PS 2 to 4 patients (median age is 75 years) provides critical reassurance that osimertinib is tolerable even in elderly and frail cohorts, with evidence of performance status improvement alongside antitumor activity[63,71]. This tolerability in functionally compromised patients further distinguishes osimertinib from cytotoxic chemotherapy and, to a lesser extent, from earlier-generation TKIs with higher rates of treatment-limiting dermatologic and gastrointestinal events.
By integrating the totality of safety evidence, several principles emerge for clinical practice. First, the overall risk and benefit profile of osimertinib is favorable and consistent across disease stages, treatment lines, and diverse patient populations, with dermatologic and gastrointestinal events being the most common but overwhelmingly manageable toxicities. Second, ILD or pneumonitis, although infrequent (1% to 4% across studies), is the principal life-threatening adverse event and demands proactive monitoring, prompt diagnostic workup upon symptom onset, and a low threshold for treatment interruption, especially in postradiation settings, East Asian populations, and heavily pretreated or ctDNA-selected programs where disease burden and prior thoracic injury may amplify risk. Third, cardiac monitoring should be incorporated into long-term treatment plans, particularly for adjuvant and consolidation therapies that extend over time. Fourth, the incremental toxicity introduced by chemotherapy combination regimens is real but manageable and must be contextualized against the magnitude of the additional efficacy benefit offered to each individual patient. Collectively, this safety evidence supports the continued expansion of the therapeutic role of osimertinib across the EGFR-mutated NSCLC continuum, with appropriate risk stratification monitoring as an essential component of the treatment paradigm.
EVIDENCE FROM REAL-WORLD STUDIES
While unusually comprehensive, the prospective clinical trial portfolio of osimertinib was necessarily conducted in selected populations meeting strict eligibility criteria, typically patients with good performance status, limited comorbidities, confirmed tissue-based molecular testing, and access to protocol-mandated follow-up. The extent to which these controlled efficacy and safety signals translate into heterogeneous clinical practice settings—where patients are older, frailer, more heavily pretreated, and managed under diverse healthcare systems—can only be addressed by large-scale real-world studies. Over the past several years, a substantial body of observational evidence has accumulated across multiple continents and clinical contexts, providing an essential complement to randomized trial data and progressively filling evidence gaps for populations underrepresented in registration programs[78-83]. Tables 4 and 5 summarize evidence from real-world studies.
Real-world evidence for osimertinib in EGFR-mutated NSCLC: study characteristics and key outcomes
| Study | Geography | Design | Clinical setting | No. of patients | Prior lines of therapy | Key efficacy outcomes | Safety highlights | Comparator Trial benchmark |
| ASTRIS[78] | Global (multi-country) | Non-interventional, prospective real-world | T790M+ post-EGFR-TKI | > 3,000 | ≥ 1 prior EGFR-TKI | ORR 57.1%; median PFS 11.1 mo; median TTD 13.5 mo | ILD/pneumonitis ~1% | AURA extension: ORR high, PFS 12.3 mo, ILD ~4%; AURA3: PFS superior to chemo |
| Korean multicenter cohort[79] | South Korea | Retrospective, multicenter | T790M+ post-EGFR-TKI | 558 | ≥ 1 prior EGFR-TKI (3rd-gen TKI excluded) | ORR 55.2%; median PFS 14.2 mo; median TTD 15.0 mo; median OS 36.7 mo | Severe AE discontinuation 1.8% (including pneumonitis) | AURA extension: PFS 12.3 mo; Korean AURA ext/AURA2: ORR 74%, DoR 9.8 mo |
| Taiwanese early-access program[81] | Taiwan | Retrospective, single-arm (early-access) | T790M+ post-EGFR-TKI | 419 | 53% ≥ 3 prior lines | ORR 32.5%; DCR 86.4%; median PFS 10.5 mo; median OS 19.0 mo | Consistent with trial data; no new signals | AURA extension: PFS 12.3 mo; LiquidLung-O C2: ORR 66.7%, PFS 8.3 mo |
| Indian tertiary center cohort[83] | India | Single-center, prospective/retrospective | 1st-line metastatic EGFR-mut | 129 | None (first-line) | ORR ~77.5%; median PFS 21.9 mo; median OS 31 mo | Manageable; consistent with trial profile | FLAURA: PFS HR 0.46 vs. 1st-gen TKIs; median PFS ~18.9 mo |
| CAPTRALung (Chinese multicenter)[80] | China | Multicenter, retrospective; propensity-score matched (1:2) | 1st-line metastatic EGFR-mut | 1,556 total (202 osi; 1,354 1st-gen TKIs) | None (first-line) | Significantly improved PFS with osimertinib vs. 1st-gen TKIs after PSM | Comparable safety profile vs. 1st-gen TKIs | FLAURA: PFS and OS superiority vs. gefitinib/erlotinib |
| Taiwanese retrospective cohort[82] | Taiwan | Single-center, retrospective | 1st-line metastatic EGFR-mut | 168 (55 osi; 113 afatinib/dacomitinib) | None (first-line) | No statistically significant PFS difference between osi and 2nd-gen TKIs | - | FLAURA: PFS HR 0.46 vs. 1st-gen TKIs; limited by small sample and short follow-up |
Concordance and contextual variation between clinical trial efficacy and real-world effectiveness of osimertinib
| Dimension | Pattern observed | Supporting data |
| Trial-to-real-world consistency (T790M+ setting) | Real-world PFS closely approximates registration trial PFS | ASTRIS PFS 11.1 mo; Korean PFS 14.2 mo vs. AURA extension PFS 12.3 mo ; |
| Trial-to-real-world consistency (1st-line setting) | First-line real-world effectiveness mirrors FLAURA results | Indian PFS 21.9 mo; CAPTRALung PSM PFS advantage vs. FLAURA PFS HR 0.46 |
| Impact of treatment-line burden | Heavier pretreatment correlates with attenuated outcomes | Taiwanese EAP (53% ≥ 3 lines): ORR 32.5%, PFS 10.5 mo, OS 19.0 mo vs. Korean (≥ 1 line): ORR 55.2%, PFS 14.2 mo, OS 36.7 mo |
| Real-world safety vs. trial safety | ILD/pneumonitis rates lower in real-world than in registration trials | ASTRIS ILD ~1%; Korean discontinuation 1.8% vs. AURA extension ILD ~4%; |
| Geographic generalizability | Consistent effectiveness across India, China, Korea, Taiwan, and global cohorts | PFS range: 10.5-21.9 mo across settings; no geography shows markedly discordant outcomes |
| Comparator context matters | Osimertinib superiority vs. 1st-gen TKIs confirmed; vs. 2nd-gen TKIs less clear on limited data | CAPTRALung: significant PFS advantage vs. 1st-gen; Taiwanese cohort: NS difference vs. afatinib/dacomitinib (small N, short follow-up) |
The largest and most geographically diverse real-world dataset comes from the ASTRIS study, a global, noninterventional program that included more than 3,000 patients with T790M-positive advanced NSCLC treated with osimertinib after progression on prior EGFR-TKIs[78]. In this heterogeneous cohort, encompassing patients from multiple countries, practice settings, and clinical profiles that would not uniformly qualify for randomized trial enrollment, osimertinib achieved an investigator-assessed ORR of 57.1%, a median PFS of 11.1 months, and a median time to treatment discontinuation of 13.5 months. These effectiveness metrics are broadly concordant with the 12.3-month median PFS and high ORR observed in the AURA phase II extension[67] and the PFS advantage demonstrated in AURA3[65], providing critical reassurance that the controlled trial findings are reproducible across the diversity of real-world practice. Equally notable was the safety profile: ILD/pneumonitis was documented in approximately 1% of the ASTRIS population[78], substantially lower than the 4% rate observed in the AURA extension[67]. While this difference likely reflects, in part, the less intensive adverse event capture inherent in observational designs, the less stringent surveillance protocols, and the potential for underreporting in routine clinical practice, the low real-world ILD incidence nevertheless provides clinicians with a practical benchmark for counseling patients about risk magnitude outside the controlled trial setting.
Regional real-world cohorts from East Asia, where EGFR-mutated NSCLC has the highest prevalence and where osimertinib utilization is most extensive, offer further granularity. A Korean multicenter retrospective study analyzed outcomes in 558 patients treated with osimertinib for T790M-positive disease after prior EGFR-TKI therapy[79]. This cohort, reflecting the spectrum of real-world clinical complexity, including varied numbers of prior treatment lines and diverse comorbidity profiles, had a median PFS of 14.2 months, an ORR of 55.2%, a median time to treatment discontinuation of 15.0 months, and a median OS of 36.7 months. The PFS of 14.2 months slightly exceeds the 12.3 months observed in the AURA extension and is notably longer than the 8.3 months reported in the plasma-only T790M-selected Liquid Lung-O Cohort 2[68], likely reflecting the favorable prognostic profile of a tissue-confirmed T790M population in a healthcare system with a well-established molecular testing infrastructure. Discontinuation of severe adverse events, including pneumonitis, occurred in 1.8% of patients, confirming the manageable safety profile in routine Korean clinical practice. A Taiwanese early-access program provided a contrasting perspective: among 419 patients treated with osimertinib for T790M-positive locally advanced or metastatic NSCLC, the outcomes were more modest, with a median PFS of 10.5 months, a median OS of 19.0 months, an ORR of 32.5%, and a disease control rate (DCR) of 86.4%[81]. Critically, this Taiwanese cohort was substantially more heavily pretreated than either the Korean cohort or the registration trial population, with 53% of patients having received three or more prior lines of therapy. The attenuated ORR (32.5% vs. 55% to 74% in less pretreated cohorts[69,79]) and shorter OS (19.0 vs. 36.7 months[79]) illustrate the expected inverse relationship between treatment-line burden and therapeutic efficacy and provide a realistic benchmark for the outcomes achievable when osimertinib is deployed in late-line, heavily pretreated settings that are common in clinical practice but poorly represented in prospective trials.
The transition to first-line real-world osimertinib data marked an important evolution in the evidence base. An Indian single-center study from a tertiary cancer center analyzed 129 consecutive patients with metastatic EGFR-mutated NSCLC who were treated with first-line osimertinib between March 2018 and May 2023[83]. Despite the resource constraints and patient demographic characteristics of a developing country’s oncologic practice, the outcomes were a striking median PFS of 21.9 months, a median OS of 31 months, and an ORR of approximately 77.5%. These figures closely parallel the FLAURA trial results (PFS HR 0.46 vs. first-generation TKIs; median PFS approximately 18.9 months in the osimertinib arm) and demonstrate that the controlled trial efficacy is achievable in a geographically and socioeconomically distinct clinical setting. The Chinese CAPTRALung multicenter database analysis provided a relatively large-scale and methodologically more rigorous first-line comparison: among 1,556 patients with advanced EGFR-mutated NSCLC (202 receiving osimertinib and 1,354 receiving first-generation TKIs), propensity score matching at a 1:2 ratio was employed to adjust for baseline covariate imbalances[80]. After matching, compared with first-generation TKIs, osimertinib significantly improved PFS, with a comparable safety profile effectively recapitulating the FLAURA findings in a real-world Chinese population and supporting the generalizability of osimertinib's first-line superiority across the region where EGFR-mutated NSCLC is most prevalent. A Taiwanese retrospective cohort study provided more equivocal results in a different comparative context: among 168 stage IIIb-IV patients treated between April 2020 and April 2023 (55, osimertinib; 113, afatinib/dacomitinib), no statistically significant difference in PFS was observed between osimertinib and second-generation EGFR-TKIs[82]. However, this study was limited by its single-center design, modest sample size, and relatively short follow-up duration, factors that collectively limit its statistical power to detect the magnitude of PFS difference demonstrated in larger trials and may not adequately capture differences in CNS relapse prevention or OS that have been the more definitive discriminating endpoints in prospective randomized data.
When the totality of real-world evidence is appraised alongside the prospective clinical trial portfolio, several overarching patterns emerge with important implications for clinical practice and future research. First, the effectiveness of osimertinib in routine practice consistently approximates, and in some cohorts closely replicates, the efficacy observed in registration trials, both in the second-line T790M-positive setting (ASTRIS median PFS 11.1 months; Korean cohort 14.2 months; vs. AURA extension 12.3 months) and in the first-line context (Indian cohort PFS 21.9 months; CAPTRALung propensity-matched PFS advantage; vs. FLAURA). This consistency across geographies, across India, China, Korea, Taiwan, and global multicountry programs and healthcare systems provides robust external validation of the randomized evidence. Second, outcomes are meaningfully influenced by treatment-line burden and patient selection: heavily pretreated populations (Taiwanese EAP: 53% ≥ 3 prior lines; PFS 10.5 months, ORR 32.5%) show attenuated benefit compared with earlier-line cohorts (Korean: PFS 14.2 months, ORR 55.2%), underscoring the importance of optimizing the sequencing and timing of osimertinib deployment. Third, the safety profile in real-world practice is consistently reassuring, with ILD or pneumonitis rates of approximately 1% to 2% (ASTRIS 1%; Korean severe adeverse event (AE) discontinuation 1.8%), lower than the 4% observed in the more intensively monitored AURA extension, and no emergence of novel safety signals despite broader and less selected patient populations. Fourth, these real-world cohorts progressively fill evidence gaps for subgroups underrepresented or excluded from pivotal trials: patients with multiple comorbidities, advanced age, complex prior treatment histories, diverse ethnic and socioeconomic backgrounds, and variable access to molecular diagnostics and follow-up infrastructure. The growing contribution of data from low- and middle-income countries is particularly valuable, as it addresses the global equity dimension of targeted therapy access and effectiveness.
Certain limitations of the real-world evidence base must, however, be acknowledged. Observational studies are inherently subject to selection bias, immortal time bias, and confounding by indication even when propensity score methods are employed. Investigator-assessed endpoints in the absence of blinded independent central review may introduce measurement bias that favors either overestimation or underestimation of treatment effects depending on the context. Adverse events captured in routine practice are typically less systematic than those captured in clinical trials, potentially underestimating the true incidence of less common but clinically significant toxicities such as ILD and cardiac events. The retrospective, single-center design of several key studies limits generalizability and statistical power. Ongoing large-scale prospective registries and pragmatic clinical trials will be essential for further refining the real-world evidence base, particularly for long-term outcomes after multiyear adjuvant or consolidation therapy, comparative effectiveness against emerging combination regimens, and safety surveillance in populations with extended osimertinib exposure. Taken together, the real-world evidence for osimertinib provides a coherent and reassuring message: the transformative efficacy demonstrated in prospective randomized trials is translatable to the complexity and diversity of routine clinical practice across global healthcare settings. This body of evidence reinforces the position of osimertinib as a central EGFR-targeted agent for real-world patients with EGFR-mutated NSCLC while simultaneously highlighting the importance of treatment-line optimization, population-specific safety monitoring, and continued data generation from underrepresented geographies and clinical subgroups. The treatment continuum according to the Sankey diagram is shown in Figure 2. Notably, Figure 2 represents a conceptual synthesis of the treatment continuum informed by the aggregate evidence base rather than a direct patient-flow analysis derived from a single dataset.
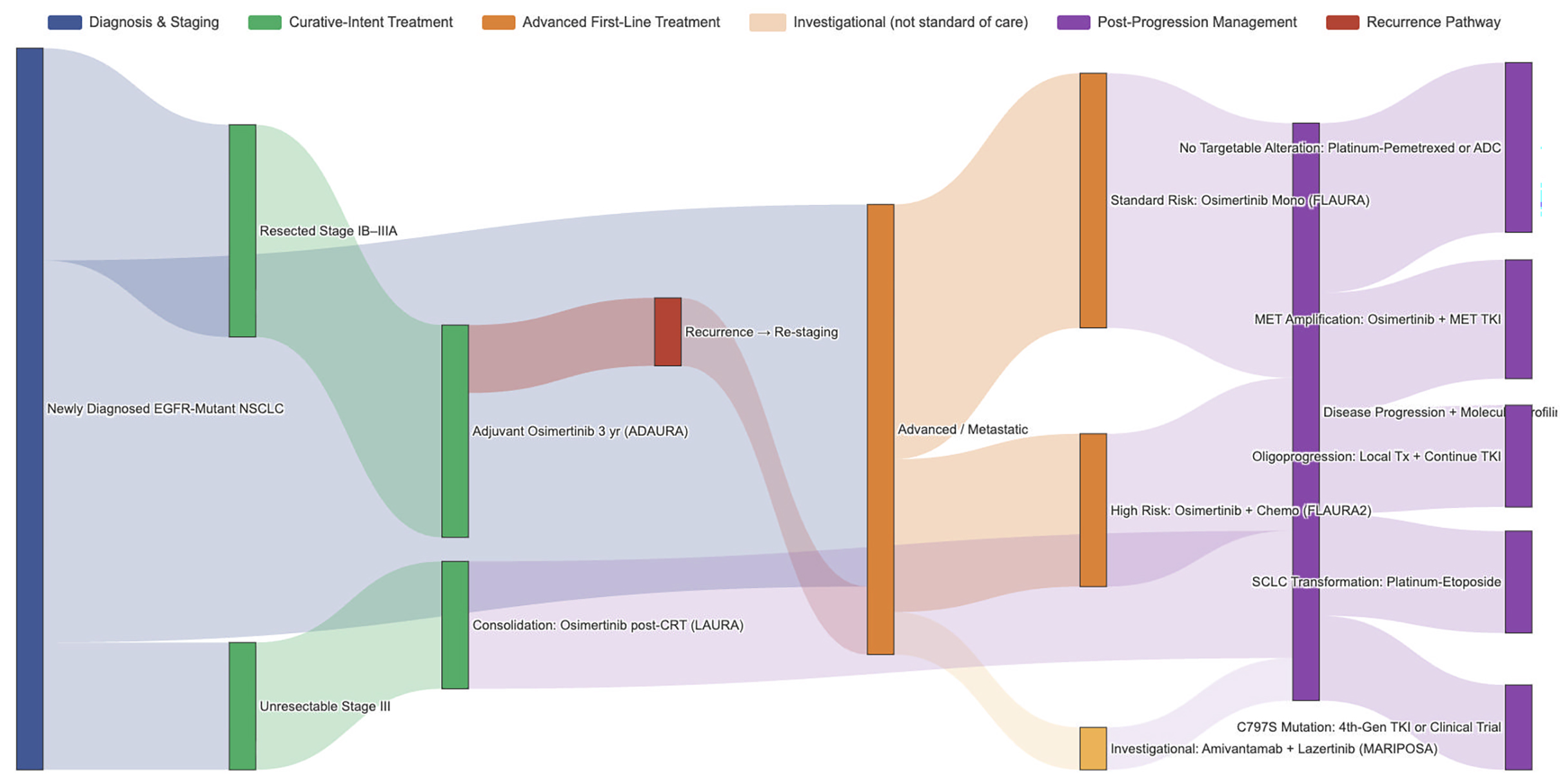
Figure 2. Conceptual treatment continuum of osimertinib across disease stages (Sankey diagram). Note: This diagram represents a synthesized, evidence-informed conceptual framework illustrating the treatment flow across clinical scenarios rather than a strictly data-derived patient-level analysis. Treatment transitions are based on current guideline recommendations and pivotal trial evidence (ADAURA, LAURA, FLAURA, FLAURA2, AURA3). The bifurcation between osimertinib monotherapy and osimertinib plus chemotherapy in the first-line advanced setting reflects the risk-stratified approach informed by FLAURA2 data, where high-risk features (e.g., TP53 comutation, high tumor burden, and L858R mutation) may favor combination therapy. Dashed lines indicate emerging or investigational pathways not yet established as the standard of care.
CHRONOLOGIC EVOLUTION
The clinical development of osimertinib traces a remarkably coherent and strategically deliberate trajectory that, over approximately one decade, has expanded the drug's therapeutic role from a narrowly indicated salvage agent to a universal backbone therapy spanning the entire EGFR-mutated NSCLC disease continuum. This evolution can be understood through three distinct strategic phases, each driven by a unifying clinical question that naturally arose from the preceding evidence.
Phase I (2013-2017): Establishing proof-of-concept in T790M-mediated resistance. The earliest phase was defined by the imperative to address T790M-mediated acquired resistance, the most common mechanism of failure of first- and second-generation EGFR-TKIs[84]. The AURA phase I/II expansion and subsequent AURA3 phase III trial established randomized superiority over platinum-pemetrexed chemotherapy, leading to global adoption as the standard second-line therapy for T790M-positive progression[65,67]. CNS-focused analyses of AURA3 revealed a pharmacologically distinctive intracranial efficacy that is central to the therapeutic efficacy of osimertinib[66,76]. During this same period, the LiquidLung-O Cohort 2 trial (Liquid biopsy in Lung cancer for Osimertinib and WJOG 8815L trials (West Japan Oncology Group study 8815L; NCT02771314) marked a parallel methodological evolution from tissue-based to plasma-based T790M detection[68,85], whereas the APOLLO study uniquely integrated CSF pharmacokinetic measurements, reframing intracranial activity from a secondary observation to a primary therapeutic attribute[77].
Phase II (2017-2020): Moving to first-line and optimizing deployment. With T790M-directed efficacy established, the logical question became whether earlier deployment could yield greater benefit. The FLAURA trial answered definitively, demonstrating both PFS and OS superiority over first-generation TKIs as first-line therapy and effecting a paradigm shift from salvage to universal frontline use[3,56]. Subsequent studies refined this deployment: the LiquidLung-O Cohort 1 trial revealed striking mutation-specific heterogeneity of benefit that challenged the assumption of uniform efficacy across EGFR mutation subtypes[57,64], and the OPEN/TORG2040 trial extended the evidence to the previously neglected poor-performance-status population[62,63]. Real-world effectiveness data from multiple countries progressively confirmed the generalizability of these findings across diverse healthcare systems (Section “EVIDENCE FROM REAL-WORLD STUDIES”).
Phase III (2020-present): Extending to curative-intent settings and combination strategies. The most transformative phase extended osimertinib into curative-intent contexts, fundamentally redefining EGFR-mutated NSCLC from a metastatic-only treatment target to a molecular disease requiring targeted intervention across the entire disease trajectory. The ADAURA trial provided the first evidence that targeted adjuvant therapy is disease-modifying and capable of improving overall survival in patients with resected EGFR-mutated NSCLC[47,50], whereas the LAURA trial established targeted consolidation after chemoradiotherapy in patients with unresectable stage III disease[55]. Neoadjuvant programs (NCT03433469, NEOS) have demonstrated the feasibility of preoperative osimertinib, although the incremental benefit over adjuvant-only strategies remains an open question to be addressed by the ongoing NeoADAURA phase III trial[52-54,86]. Paralleling this stage-based expansion, the mutation spectrum broadened through the KCSG-LU15-09 and UNICORN trials for uncommon mutations[70], and combination intensification strategies matured, with FLAURA2 establishing the foundation for risk-stratified frontline treatment selection[60]. This chronological evolution is illustrated in Figure 3, which maps the key milestone trials to their respective strategic phases.
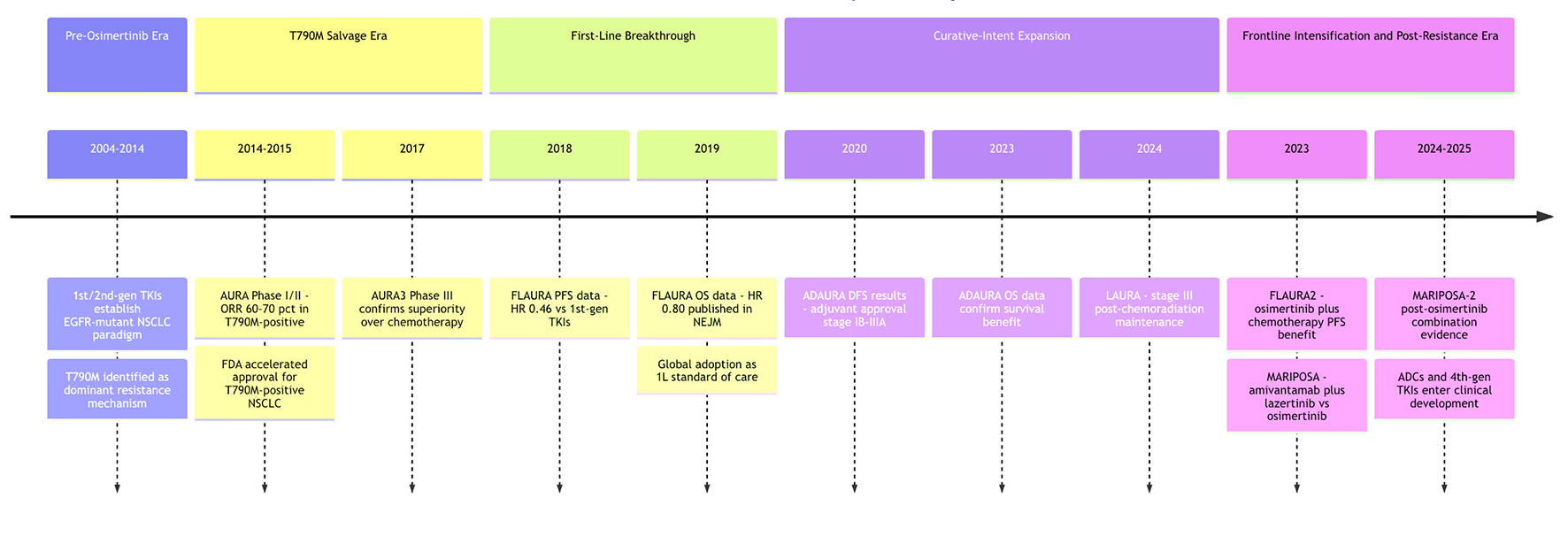
Figure 3. Timeline of Milestone trials of osimertinib in lung cancer.
RESISTANCE MECHANISMS AND THE POST-OSIMERTINIB LANDSCAPE
Despite the transformative efficacy of osimertinib across clinical settings, acquired resistance remains an inevitable clinical reality that ultimately limits the duration of benefit for virtually all patients, and a growing body of narrative reviews has comprehensively mapped the complex, heterogeneous landscape of resistance biology that underpins this challenge. Multiple dedicated reviews, most notably those by Lazzari et al. (2020)[20], He et al. (2021)[45], and Nicoś et al. (2025)[87], have classified resistance mechanisms into three broad categories: (1) on-target EGFR-dependent alterations, principally the tertiary C797S mutation in exon 20, which disrupts the covalent binding site of osimertinib and accounts for 0%-29% of resistance cases depending on the series; (2) off-target bypass pathway activation, including MET amplification (7%-24%), HER2 amplification, oncogenic fusions involving RET, ALK, FGFR, and other partners (1%-10%), and downstream signaling alterations in PIK3CA and RAS/MAPK pathways; and (3) histological transformation, most notably the phenotypic switch from NSCLC to SCLC, which occurs in 2%-15% of cases and results in a fundamentally altered treatment paradigm. A critically important insight emerging from these syntheses is that resistance patterns differ substantially depending on the line of therapy in which osimertinib is administered: first-line resistance tends to exhibit greater molecular heterogeneity with fewer on-target EGFR mutations and a greater proportion of bypass and transformation events, whereas second-line resistance after prior first/second-generation TKIs more frequently involves EGFR-dependent mechanisms, including C797S, a distinction with direct implications for resistance monitoring strategies and subsequent treatment selection. The heterogeneity and clinical unpredictability of bypass-mediated resistance are illustrated by the case reported by Yamaguchi et al. (2024), in which a patient with EGFR L858R-positive NSCLC developed acquired EML4-ALK variant 3a/b rearrangement after 15 months of first-line osimertinib, notably the first reported instance of ALK fusion arising under first-line osimertinib selective pressure independent of T790M, with the synchronous coexistence of two canonically mutually exclusive oncogenic drivers in the same tumor[88]. The limited efficacy of subsequent brigatinib monotherapy in this dual-driver context suggests that single-agent targeting of only one pathway is insufficient for cross-driver resistance scenarios, underscoring the need for combination strategies and dedicated clinical trials in this molecularly defined subpopulation. This case serves as a reminder that resistance can involve unexpected oncogenic driver switching beyond the reach of population-level profiling, reinforcing the imperative for comprehensive genomic assessment, incorporating both tissue rebiopsy and liquid biopsy at the time of disease progression. Recognizing the central role of real-time molecular characterization in navigating this complexity, Ntzifa et al. (2024)[89] provided a dedicated review of liquid biopsy strategies during osimertinib treatment, establishing a framework for longitudinal ctDNA and circulating tumor cell (CTC) monitoring that enables noninvasive detection of emergent resistance mechanisms, tracking of clonal evolution under therapeutic pressure, and timely adaptation of treatment, which is applicable across first-line, adjuvant, neoadjuvant, and unresectable stage III contexts where osimertinib is now employed. The therapeutic translation of resistance biology into actionable postosimertinib treatment pathways remains, however, at a relatively early stage of evidence maturity: Zhang et al. (2025)[90] conducted the first network meta-analysis of subsequent-line regimens after EGFR-TKI resistance, comparing the efficacy and safety of distinct postprogression strategies, including chemotherapy, immunotherapy combinations, and targeted approaches. Notwithstanding this, the heterogeneity of the included populations, the diversity of resistance mechanisms within trial cohorts, and the absence of resistance-mechanism-stratified randomization in most contributing studies limit the precision with which these network meta-analysis (NMA) estimates can be applied to individual patients with molecularly defined resistance profiles. Nicoś et al. (2025)[87] further surveyed the emerging therapeutic armamentarium designed to overcome osimertinib resistance, including fourth-generation EGFR-TKIs engineered to circumvent C797S (such as BLU-945 and BLU-525), bispecific antibodies (amivantamab), antibody‒drug conjugates (patritumab deruxtecan and datopotamab deruxtecan), MET-targeted combinations, and other mechanism-informed strategies currently under clinical investigation. However, none of these approaches has yet achieved the level of evidence supporting a definitive standard-of-care recommendation. Several of these strategies have nonetheless progressed beyond preclinical rationale to generate early-phase clinical evidence that warrants further discussion. Among fourth-generation EGFR TKIs, BLU-945, an allosteric inhibitor designed to overcome C797S while maintaining activity against the original sensitizing mutation, has demonstrated preliminary antitumor activity, including confirmed partial responses in C797S-positive patients in the phase I/II SYMPHONY trial[87]. Among bispecific antibodies, the MARIPOSA-2 trial demonstrated that amivantamab plus lazertinib plus chemotherapy significantly improved PFS over chemotherapy alone in patients who progressed on osimertinib (median PFS 8.3 vs. 4.2 months; HR 0.44), providing the first randomized evidence for a postosimertinib combination regimen[91]. Among antibody-drug conjugates, patritumab deruxtecan (HER3-DXd) achieved a confirmed ORR of 29.8% (95%CI: 23.9-36.2), a median duration of response of 6.4 months, and a median PFS of 5.5 months in heavily pretreated EGFR-mutant NSCLC patients in the HERTHENA-Lung01 phase II trial, with efficacy observed across diverse mechanisms of EGFR-TKI resistance and a confirmed CNS ORR of 33.3% in patients with nonirradiated brain metastases[92], while datopotamab deruxtecan (Dato-DXd, targeting trophoblast cell-surface antigen 2 (TROP2)) is under evaluation in the TROPION-Lung05 and TROPION-Lung15 trials with preliminary signals of activity[42,93]. Among MET-targeted combinations, savolitinib combined with osimertinib achieved a confirmed ORR of up to 62% in MET-amplified osimertinib-resistant patients in the TATTON trial[94], and tepotinib plus osimertinib demonstrated similar activity in the INSIGHT 2 trial[95]. These data, while predominantly from single-arm phase I/II studies, collectively support a mechanism-informed, biomarker-guided approach to postosimertinib treatment selection and underscore the critical importance of comprehensive genomic profiling at the time of resistance to match each patient’s molecular profile to the most appropriate emerging strategy. Collectively, these resistance-focused reviews provide the essential conceptual scaffolding for interpreting survival endpoints across trials and treatment eras: as the proportion of patients receiving first-line osimertinib increases and the postosimertinib treatment landscape evolves, the nature and frequency of resistance mechanisms encountered in clinical practice will shift, cross-trial comparability of overall survival will become increasingly contingent on postprogression therapies received, and the design of future evidence syntheses, whether meta-analyses or network meta-analyses, will need to explicitly account for resistance biology, liquid biopsy-guided treatment adaptation, and the sequential therapeutic context in which osimertinib is deployed[20,45].
DISCUSSION
The evidence synthesized in this review establishes osimertinib as the most extensively validated targeted agent in the history of thoracic oncology, with a prospective clinical trial portfolio spanning the full disease continuum of EGFR-mutated NSCLC, from resectable early-stage and unresectable locally advanced to advanced metastatic disease. This portfolio also encompasses multiple molecular subsets, diverse patient populations, and both monotherapy and combination approaches.
Contextualizing primary evidence within the existing synthesis landscape
The primary trial evidence presented in this review must be interpreted against a substantial body of published evidence syntheses, pairwise meta-analyses, network meta-analyses, and subgroup-focused systematic reviews that have quantified osimertinib’s comparative effectiveness across clinical settings. Rather than recapitulating each synthesis in detail, we focus here on the key areas of consensus and unresolved debate that are most relevant to current clinical decision-making.
The most robust and internally consistent finding across all published pairwise meta-analyses is the superiority of osimertinib over earlier-generation EGFR-TKIs and platinum-based chemotherapy in advanced EGFR-mutant NSCLC. Multiple independent analyses encompassing between 1,848 and 3,335 patients from 6 to 10 randomized controlled trials have uniformly demonstrated significant advantages in terms of the objective response rate, disease control rate, progression-free survival, and overall survival, with concurrent reductions in grade ≥ 3 adverse events[30,33,34,96,97]. This convergence of evidence across different analytical teams, timepoints, and methodological approaches, from Chen et al. (2018)[33] through Huang et al. (2019)[34] and Li et al. (2022)[30] to the most recent third-generation TKI-focused synthesis by Lin et al. (2026)[97], leaves little residual uncertainty regarding osimertinib’s comparative efficacy in the advanced setting. Li et al. (2022) mention incorporating CNS progression-free survival as a coprimary meta-analytic endpoint, one of the few broad syntheses to formally quantify the intracranial advantage of osimertinib at the level of evidence synthesis[30]. One methodological outlier warrants acknowledgment: Zhao et al. (2024) reported pooled analyses in which gefitinib/erlotinib occasionally appeared to favor PFS/OS over osimertinib monotherapy[39]. This finding is discordant with the totality of evidence from the head-to-head FLAURA trial and all other published meta-analyses. This discrepancy likely reflects differences in trial selection criteria, regional trial composition, the inclusion of Chinese database studies, and statistical weighting approaches and should be interpreted with caution rather than accepted as evidence of genuine therapeutic equivalence.
Network meta-analyses have extended the comparative evidence base beyond head-to-head trial pairs, enabling indirect comparisons across agents never evaluated against one another in randomized designs. The foundational NMAs, published between 2019 and 2020, consistently ranked osimertinib monotherapy at or near the top of first-line efficacy hierarchies for both PFS and OS, with safety profiles comparable to or better than those of first-generation TKIs[37,98,99]. This consensus positioning provided the quantitative underpinning for osimertinib’s rapid guideline adoption as the preferred first-line agent globally. However, as the first-line landscape has expanded to include combination regimens and additional third-generation TKIs, the NMA evidence has become more nuanced. Two important findings have emerged. First, mutation-specific treatment selection has gained quantitative support: Xie et al. (2021)[100] and Chan et al. (2022)[101] demonstrated that while osimertinib consistently ranks highest for PFS in patients with exon 19 deletion, those harboring L858R may derive comparable or superior benefits from TKI-plus-chemotherapy combinations or dacomitinib, highlighting the importance of genotype-stratified decision-making[100,101]. Second, the emergence of additional third-generation agents, such as furmonertinib, aumolertinib, and others, has introduced intraclass competition: Du et al. (2025), in the first dedicated NMA within the third-generation TKI class, reported that while all third-generation agents were superior to first-generation TKIs, furmonertinib ranked highest for PFS and aumolertinib for intracranial control, with osimertinib slightly lower in these specific rankings[102]. Zhang et al. (2024), who analyzed 35 randomized controlled trials (RCTs) across 21 regimens, further demonstrated that third-generation TKI-based combinations achieved the highest overall PFS rankings, surpassing all monotherapy options[103]. These evolving NMA findings signal a transition from a landscape in which osimertinib monotherapy was the uncontested first-line choice to one requiring increasingly individualized treatment selection on the basis of mutation subtype, CNS status, disease burden, and tolerability preferences.
The intracranial efficacy of osimertinib was quantified through dedicated pooled analyses that complement the trial-level CNS data reviewed in Section "EFFICACY OF THE CENTRAL NERVOUS SYSTEM". Wang et al. (2020)[35] and Erickson et al. (2020)[104] provided convergent pooled estimates of CNS objective response rates of approximately 60% to 65% and CNS disease control rates exceeding 90%, confirming that the intracranial activity of osimertinib is not an isolated observation from individual trials but rather a reproducible and quantitatively substantial therapeutic effect[35,104]. Liu et al. (2021), in a Bayesian NMA of treatment modalities for NSCLC patients with brain metastases, reported that compared with first- and second-generation TKIs, radiotherapy, and chemotherapy, osimertinib significantly increased PFS, although the increase in OS was less pronounced, a finding consistent with the availability of effective subsequent therapies that decrease OS differences across treatment arms[105]. A critical nuance emerged from Ma et al. (2024), who specifically analyzed first-line treatment in patients with EGFR-mutant NSCLC with brain metastases and reported that compared with first-generation TKIs, third-generation TKI monotherapy did not significantly improve overall survival but that indirect evidence favored third-generation TKI plus chemotherapy as the most efficacious strategy for both OS and PFS in this CNS-heavy population[106]. These findings challenge the long-standing assumption that third-generation TKI monotherapy universally dominates OS outcomes in brain-metastatic patients and provide a compelling, evidence-synthesis-level rationale for combination approaches in this high-risk subgroup. Mei et al. (2025), in the largest brain metastasis-stratified NMA to date encompassing 37 RCTs and 24 interventions, corroborated these findings by demonstrating that compared with other TKI monotherapy regimens, osimertinib plus chemotherapy significantly improved PFS, with the advantage being particularly pronounced in brain metastasis-positive cohorts[107]. Beyond parenchymal brain metastases, leptomeningeal metastases represent a particularly devastating complication for which osimertinib has emerged as the most extensively studied systemic agent. Wen et al. (2023), in the largest leptomeningeal-metastases-specific pooled analysis to date, reported clinically meaningful response and disease control rates with encouraging one-year survival across both standard- and high-dose cohorts[108]. Bian et al. (2024), using individual patient-data meta-analyses across EGFR-TKI generations, reported that compared with earlier-generation TKIs, osimertinib was associated with improved CNS-PFS and OS in previously treated leptomeningeal disease, although superiority was less clearly established in TKI-naïve leptomeningeal patients[109], a finding that underscores the importance of treatment sequencing even within the CNS-specific domain.
A critically important insight that has crystallized across subgroup-focused systematic reviews is that the clinical benefit of osimertinib is not uniform across the EGFR mutation spectrum but is strongly conditioned on the underlying molecular context. In the T790M-positive post-TKI population, the original regulatory indication, confirmed strong and durable efficacy through pooled analysis of more than 1,050 patients[41]. Yi et al. (2022) extended this analysis to T790M-stratified cohorts and revealed a clinically important gradient: T790M-positive patients derived the greatest benefit, T790M-unknown patients showed intermediate responses, and T790M-negative patients exhibited limited to poor efficacy[110]. This gradient provides the first quantitative framework for nuanced post-TKI decision-making and underscores the imperative of accurate T790M assessment through tissue- or plasma-based assays. With respect to uncommon EGFR mutations, Priantti et al. (2024) provided the most granular pooled data to date through a systematic review and single-arm meta-analysis encompassing 594 patients across 15 studies, demonstrating clinically meaningful but heterogeneous activity across mutation subtypes with a safety profile consistent with that observed for classical mutations[40,111]. By integrating structural biology data with clinical data, Song and Yang (2022) complemented these quantitative findings to explain why certain uncommon variants respond favorably to osimertinib, while others confer intrinsic resistance[112]. Taken together, these subgroup-focused syntheses carry a critical methodological implication: broad conclusions about osimertinib efficacy derived from pooled meta-analyses or NMAs must be carefully qualified by mutation subtype, as failure to account for this molecular heterogeneity risk obscures clinically meaningful differences in therapeutic benefit.
The meta-analytic evidence on combination strategies delivers a decisive and bifurcated message. With respect to the osimertinib-plus-bevacizumab combination, two independent meta-analyses reported largely negative conclusions: (1) Zhou et al. (2024), who pooled four RCTs with 390 patients, reported no improvement in PFS, OS, or ORR with increased VEGF-related toxicity[113]; and (2) Yao et al. (2024), who studied 10 RCTs with 824 patients, reported similar equivocal efficacy gains offset by additional toxicity burden[114]. These findings, echoed by broader NMAs that rarely rank bevacizumab-containing osimertinib regimens at the top of efficacy hierarchies[98,103,115], provide a robust evidence-synthesis basis for discouraging the routine addition of bevacizumab to osimertinib outside of clinical trials. In stark contrast, the combination of osimertinib with platinum-pemetrexed chemotherapy has emerged as a genuinely transformative escalation strategy. Prospective CNS-specific analysis from the phase III FLAURA2 trial demonstrated that compared with osimertinib alone, the combination significantly improved both systemic and intracranial progression-free survival, providing the first high-quality randomized evidence that combination chemotherapy can meaningfully augment the already substantial CNS activity of osimertinib. These trial-level findings are strongly supported by multiple NMAs identifying TKI-plus-chemotherapy combinations as the highest-ranked first-line strategies, particularly in brain metastasis-positive populations[103,107]. This trade-off, a predictable increase in hematological and gastrointestinal toxicity, necessitates careful patient selection. In aggregate, the evidence-synthesis landscape now supports a risk-stratified approach: osimertinib monotherapy for standard-risk patients and osimertinib plus platinum-pemetrexed for those with brain metastases, high systemic disease burden, or other high-risk features, indicating a decisive shift from the monotherapy-first paradigm toward regimen-level optimization.
The accumulated meta-analytic evidence firmly establishes the systemic efficacy and safety superiority of osimertinib over earlier-generation TKIs, its unparalleled CNS activity, and its expanding but context-dependent role in combination strategies. The current frontier of evidence synthesis is no only whether osimertinib is effective but also how to optimally deploy it across disease stages, CNS status, molecular subtypes, and combination regimens while navigating an increasingly competitive third-generation TKI ecosystem. Future evidence will integrate more granular biomarker-defined subgroups, maturing combination trial data, and the rapidly evolving postosimertinib treatment landscape to continue guiding precision-medicine decision-making for patients with EGFR-mutant NSCLC.
Discussion of main evidence
The most consequential finding from the collective trial portfolio is the demonstration that osimertinib confers not only progression-free survival advantages, which, while clinically meaningful, are susceptible to confounding by postprogression therapies and crossover but also definitive overall survival benefits in the two settings where this endpoint has been most rigorously assessed. In the first-line metastatic context, FLAURA confirmed the superiority of OS over first-generation EGFR-TKIs despite substantial crossover from the control arm, indicating that the true magnitude of survival benefit is likely underestimated by the intention-to-treat analysis. In the adjuvant setting, ADAURA demonstrated a statistically significant OS advantage that confirmed the disease-modifying potential of adjuvant osimertinib, a finding that is particularly striking given that patients in the placebo arm had access to effective therapies, including osimertinib, at the time of recurrence and that the OS benefit therefore reflects a genuine disease-modifying effect of early targeted intervention rather than simply delayed access to active treatment. Together, these OS results transform the clinical rationale for osimertinib from one of disease control maximization to one of cure-rate enhancement in early-stage disease and survival prolongation in metastatic disease, a distinction that has profound implications for treatment sequencing, patient counseling, and healthcare resource allocation. LAURA’s dramatic PFS prolongation, which is the greatest reported for any consolidation strategy in unresectable stage III NSCLC, awaits mature OS data to complete this picture, but the magnitude of the PFS gain and the high unmet need in this population strongly suggest that OS benefit will ultimately be demonstrated.
A second critical theme is the role of CNS disease control as a therapeutically decisive and pharmacologically unique property of osimertinib. Across every clinical setting evaluated, from intracranial response in T790M-positive brain metastases (AURA3 CNS analysis[76]; APOLLO[77]) through reduced CNS progression in first-line therapy (FLAURA[3,56,58]) to prevention of CNS relapse after curative resection (the CNS DFS benefit demonstrated in ADAURA[48,49]) and after chemoradiotherapy (LAURA[55]), osimertinib has demonstrated a consistency of intracranial benefit that is unmatched by any other systemic anticancer agent in this disease. The clinical significance of this CNS activity extends beyond conventional survival endpoints: prevention of brain metastases preserves neurocognitive function, functional independence, and quality of life in ways that are incompletely captured by PFS or OS analyses but are of paramount importance to patients. The progressive formalization of CNS endpoints across the osimertinib development program from exploratory subanalyses in AURA3[76] to protocol-specified secondary endpoints in ADAURA[48,49] reflects the field's growing recognition that CNS relapse is not merely a component of disease progression but a qualitatively distinct clinical event that merits dedicated assessment and therapeutic targeting. Future trials should incorporate CNS-specific endpoints as standard design elements, and clinical practice guidelines should explicitly consider CNS risk stratification when treatment intensity is recommended.
The mutation-specific heterogeneity of osimertinib efficacy represents a third theme with important clinical and biological implications. The consistent superiority of exon 19 deletion over L858R in terms of both the ORR and PFS, which is strongly illustrated by the striking disparity in outcomes between ex19del and L858R patients in the Liquid Lung-O Cohort 1 trial[64]) and corroborated across FLAURA and multiple other datasets[3,56], reflects the intrinsic biological differences between these mutation subtypes, which likely involve differential EGFR dimerization kinetics, signaling output, and sensitivity to irreversible covalent inhibition. For uncommon EGFR mutations, the phase II evidence from the KCSG-LU15-09 trial[70] and the superior outcomes for G719X-compound mutations identified in pooled analyses[73] support the clinical utility of osimertinib for several major uncommon genotypes while simultaneously revealing the limitations of a one-size-fits-all approach. The UNICORN trial[71,72] extends this evidence to the first-line, untreated setting, but larger, prospectively stratified studies that can power subgroup analyses by individual uncommon mutation types and compound mutation combinations are urgently needed. For exon 20 insertions, the limited activity observed at standard dosing in the LU17-19 trial[74] appropriately directed clinical development toward exon 20-specific agents and underscores that molecular precision in EGFR-mutated NSCLC extends beyond simply identifying EGFR mutations to characterize the specific structural and functional consequences of each variant. As genomic profiling becomes more granular, incorporating comutations in TP53, RB1, PIK3CA, and other genes that influence prognosis and resistance[116], the next generation of clinical trials must be designed to accommodate this molecular complexity, moving toward mutation-stratified and comutation-stratified enrollment and analysis.
The question of treatment intensification—specifically, whether combining osimertinib with platinum-pemetrexed chemotherapy offers sufficient incremental benefit to justify the additional toxicity—represents perhaps the most pressing unresolved clinical question in the field. Compared with osimertinib monotherapy, FLAURA2 treatment significantly improved PFS[59], and a final OS analysis has been reported[60]. The interpretation of these data will critically shape frontline treatment strategies. If the OS benefit is confirmed and clinically meaningful, combination therapy may become the preferred approach for molecularly or clinically defined high-risk patients—such as those with high tumor burden, TP53 comutations, L858R mutations, or baseline CNS-negative disease with high systemic metastatic load. If, however, the increase in OS is modest or absent despite the increase in PFS, the additional myelosuppression, nausea, fatigue, and logistical burden documented in FLAURA2 and OPAL[59-61] may favor continued monotherapy for most patients, with the combination reserved for carefully selected subgroups. This decision calculus will necessarily incorporate patient-reported outcomes, cost-effectiveness analyses, and the availability of effective postprogression therapy dimensions that are incompletely addressed by the current evidence but are essential for real-world treatment optimization. Beyond chemotherapy, emerging combination strategies incorporating antiangiogenic agents, MET-directed therapies, and antibody-drug conjugates[42,117,118] are poised to address the heterogeneous resistance mechanisms that inevitably emerge during osimertinib therapy, and rational, biomarker-guided selection of combination partners represents a high-priority research direction.
The management of acquired resistance to osimertinib itself constitutes a rapidly evolving and critically important domain. As first-line osimertinib use becomes universal, the resistance landscape has shifted fundamentally: T790M-mediated resistance, which drives the initial development of osimertinib, is now rarely encountered in the postfirst-line osimertinib setting and is replaced by a heterogeneous array of mechanisms, including on-target EGFR alterations (C797S, L718Q), bypass pathway activation (MET amplification, HER2 amplification), downstream signaling dysregulation (PIK3CA, RAS-MAPK pathway), and histologic transformation to small cell lung cancer or squamous cell carcinoma[20,116,119]. This mechanistic diversity presents both a challenge, as no single postosimertinib strategy is likely to be universally effective, and an opportunity, as the expanding therapeutic armamentarium now includes bispecific antibodies (amivantamab-lazertinib[120]), antibody‒drug conjugates targeting TROP2 and HER3[42,118], and next-generation EGFR-TKIs designed to overcome C797S[121]. The integration of serial ctDNA monitoring to detect emergent resistance mechanisms in real time, coupled with molecular-guided therapeutic switching, represents the most promising paradigm for postosimertinib treatment optimization, but prospective validation of ctDNA-guided algorithms remains an urgent unmet need.
The perioperative application of osimertinib raises a distinct set of strategic questions that the current evidence base has only begun to address. While ADAURA has unequivocally demonstrated the value of the adjuvant osimertinib[47-50], the optimal integration of neoadjuvant, adjuvant, and potentially perioperative targeted therapy remains undefined. The modest pathologic response rates observed in neoadjuvant-only osimertinib trials[52-54], which are lower than those achieved with neoadjuvant chemoimmunotherapy in unselected NSCLCs, raise the question of whether neoadjuvant TKI therapy adds incremental benefit over adjuvant-only strategies or whether combination neoadjuvant approaches (osimertinib plus chemotherapy, as evaluated in NeoADAURA[86]) are needed to achieve the depth of the pathologic response associated with improved long-term outcomes. Equally important is the question of adjuvant treatment duration: the 3-year fixed duration in ADAURA was empirically selected, and it remains unknown whether shorter courses might suffice for patients achieving ctDNA-negative MRD status or whether longer courses are needed for those with persistent molecular disease. ctDNA-guided adaptive adjuvant strategies for increasing the efficacy of combination therapy for MRD-positive patients and de-escalating to observe for MRD-negative patients represent a conceptually attractive but as yet unvalidated approach that could simultaneously optimize efficacy and minimize unnecessary treatment exposure[29].
The real-world evidence reviewed herein provides substantial reassurance regarding the external validity of the prospective trial findings, with effectiveness metrics across global cohorts consistently approximating the registration trial benchmarks. The safety profile in routine practice appears, if anything, more favorable than that observed in clinical trials, with ILD/pneumonitis rates of approximately 1%-2% in real-world series, compared with 4% in the more intensively monitored AURA extension; however, this discrepancy likely reflects differences in adverse event capture methodology rather than true risk reduction. Importantly, the real-world data also reveal clinically relevant patterns not fully appreciated in controlled trials: the strong inverse relationship between treatment-line burden and therapeutic efficacy, as illustrated by the attenuated outcomes in the heavily pretreated Taiwanese early-access cohort compared with earlier-line populations, underscores the importance of deploying osimertinib at the earliest appropriate disease stage rather than reserving it for later lines. This principle is now embedded in international guidelines but continues to encounter practical barriers related to molecular testing access, diagnostic turnaround time, and healthcare system logistics in many countries.
Several limitations of the evidence base as a whole warrant acknowledgment. First, the majority of pivotal trials enrolled patients with the two most common EGFR mutations (exon 19 deletion and L858R), and the evidence for uncommon mutations, while growing, remains limited to relatively small phase II studies that lack the statistical power to support definitive mutation-specific conclusions. Second, the exclusion of patients with symptomatic or unstable CNS disease from most trials means that the intracranial efficacy data apply most directly to patients with asymptomatic or treated brain metastases, and prospective evidence for osimertinib activity in patients with active, symptomatic CNS disease remains sparse. Third, the long-term consequences of multiyear osimertinib exposure, including cumulative cardiac toxicity, as well as the durability of benefit after treatment discontinuation, are incompletely characterized and will require ongoing surveillance through registries and extended follow-up analyses. Fourth, the absence of mature OS data from several important trials (LAURA, FLAURA2 final interpretation pending, OPAL) means that the survival impact of osimertinib in these settings remains to be definitively established. Fifth, the comparative effectiveness of osimertinib vs. emerging therapeutic platforms, particularly amivantamab-lazertinib combination therapy, which has shown promising activity in the MARIPOSA trial, has not been prospectively evaluated in head-to-head designs, representing a critical evidence gap as the first-line treatment landscape becomes increasingly complex.
Looking forward, the research agenda for osimertinib and EGFR-directed therapy more broadly is poised to evolve along several convergent trajectories. Biomarker-integrated trial designs that stratify patients by EGFR mutation subtype, comutational context, and ctDNA dynamics will enable increasingly precise treatment selection and adaptive management strategies. Perioperative approaches will likely move toward integrated neoadjuvant-plus-adjuvant regimens, guided by pathologic and molecular response assessments, with ctDNA-based MRD monitoring serving as the arbiter of treatment duration and intensity. Combination strategies targeting resistance mechanisms, including MET amplification, C797S mutation, PIK3CA/AKT pathway activation, and histologic transformation, will expand the therapeutic armamentarium for postosimatinib management. The growing contribution of real-world evidence from low- and middle-income countries will address the global equity dimension of targeted therapy access and outcomes. The continued maturation of OS data from LAURA, FLAURA2, and ongoing adjuvant and neoadjuvant programs will provide the definitive evidence needed to optimize treatment across every stage and clinical context[122,123]. The evidence reviewed here provides the most comprehensive foundation to date for this next phase of EGFR-directed precision oncology, a foundation built on an extraordinary breadth of prospective data and real-world experience that, collectively, supports the position of osimertinib as the indispensable therapeutic backbone for EGFR-mutated lung cancer across the entirety of its natural history[124-126].
CONCLUSIONS
Osimertinib has been established as a central EGFR-targeted agent across the full spectrum of early-stage, locally advanced, unresectable and metastatic EGFR-mutated NSCLC. Its clinical development program, encompassing multiple definitive phase III RCTs and complementary phase II studies across diverse settings, populations, and molecular subsets, represents one of the most comprehensive targeted therapy evidence bases in oncology. The consistent demonstration of efficacy (PFS/DFS and OS benefits), clinically significant CNS disease control, and a favorable and predictable safety profile collectively support the role of osimertinib as the backbone of EGFR-directed therapy. Ongoing and future studies addressing combination strategies, mutation-granular evidence, perioperative optimization, resistance management, and real-world implementation will further refine its use and maximally realize the promise of precision oncology for patients with EGFR-mutated lung cancer.
DECLARATIONS
Authors’ contributions
Conceived the methods of the study, performed the database search, article selection, and data extraction processes: Tang X, Zhu Y, Yan J
Performed the statistical analysis and drafted the manuscript: Tang X, Zhu Y
Conceived the methods of the study, performed the database search, article selection, and data extraction processes, and drafted the manuscript: Wu H, Chen Y, Liu Y, Tang H, Wang W
Helped draft the manuscript: Wang W, Wang Z
Reviewed and edited the manuscript in accordance with the reviewers' comments: Yan J
All the authors read and approved the manuscript.
Availability of data and material
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This work was supported by the National Natural Science Foundation of China (Nos. 32370628, 92159302, 32170592); the Science and Technology Project of Sichuan (Nos. 2022ZDZX0018, 2023NSFSC004,2024NSFSC0402); the Key R&D Support Plan of Chengdu Science and Technology Bureau (No. 2023-YF09-00039-SN); and the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (No. ZYGD22009).
Conflicts of interest
Wang W is a Section Editor of the Journal of Translational Genetics and Genomics. Wang W was not involved in any stage of the editorial process, including reviewer selection, manuscript handling, or decision-making, while the other authors have declared that they have no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Jakobsen E, Olsen KE, Bliddal M, Hornbak M, Persson GF, Green A. Forecasting lung cancer incidence, mortality, and prevalence to year 2030. BMC Cancer. 2021;21:985.
2. Araki T, Kanda S, Horinouchi H, Ohe Y. Current treatment strategies for EGFR-mutated non-small cell lung cancer: from first line to beyond osimertinib resistance. Jpn J Clin Oncol. 2023;53:547-61.
3. Soria J, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378:113-25.
4. Cross DA, Ashton SE, Ghiorghiu S, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4:1046-61.
5. Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31:3327-34.
6. Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239-46.
7. Zhou C, Wu Y, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735-42.
8. Goss G, Tsai C, Shepherd FA, et al. Osimertinib for pretreated EGFR Thr790Met-positive advanced non-small-cell lung cancer (AURA2): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2016;17:1643-52.
9. Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11:121-8.
10. Wu Y, Zhou C, Hu C, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15:213-22.
11. Ballard P, Yates JW, Yang Z, et al. Preclinical comparison of osimertinib with other EGFR-TKIs in EGFR-mutant NSCLC brain metastases models, and early evidence of clinical brain metastases activity. Clin Cancer Res. 2016;22:5130-40.
12. Gomatou G, Syrigos N, Kotteas E. Osimertinib resistance: molecular mechanisms and emerging treatment options. Cancers. 2023;15:841.
13. Tao W, Tang X, Jiao X, et al. Effectiveness of interventions for increasing lung cancer screening uptake: a systematic review and meta-analysis of randomized clinical trials. Prev Med. 2026;203:108489.
14. Tang X, Pang Y, Zhu P, et al. Cell apoptosis and glucocorticoid-induced osteonecrosis. Med Res. 2025;1:207-25.
15. Fu K, Xie F, Wang F, Fu L. Therapeutic strategies for EGFR-mutated non-small cell lung cancer patients with osimertinib resistance. J Hematol Oncol. 2022;15:173.
16. Piper-Vallillo AJ, Sequist LV, Piotrowska Z. Emerging treatment paradigms for EGFR-mutant lung cancers progressing on osimertinib: a review. J Clin Oncol. 2020;38:2926-36.
17. Lee J, Piotrowska Z, Soo R, Cho BC, Lim SM. Combatting acquired resistance to osimertinib in EGFR-mutant lung cancer. Ther Adv Med Oncol. 2022;14:17588359221144099.
18. Blaquier JB, Ortiz-Cuaran S, Ricciuti B, Mezquita L, Cardona AF, Recondo G. Tackling osimertinib resistance in EGFR-mutant non-small cell lung cancer. Clin Cancer Res. 2023;29:3579-91.
19. Leonetti A, Sharma S, Minari R, Perego P, Giovannetti E, Tiseo M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br J Cancer. 2019;121:725-37.
20. Lazzari C, Gregorc V, Karachaliou N, Rosell R, Santarpia M. Mechanisms of resistance to osimertinib. J Thorac Dis. 2020;12:2851-8.
21. Bertoli E, De Carlo E, Del Conte A, et al. Acquired resistance to osimertinib in EGFR-mutated non-small cell lung cancer: how do we overcome it? Int J Mol Sci. 2022;23:6936.
22. Zeng Y, Yu D, Tian W, Wu F. Resistance mechanisms to osimertinib and emerging therapeutic strategies in nonsmall cell lung cancer. Curr Opin Oncol. 2022;34:54-65.
23. Le X, Puri S, Negrao MV, et al. Landscape of EGFR-dependent and -independent resistance mechanisms to osimertinib and continuation therapy beyond progression in EGFR-mutant NSCLC. Clin Cancer Res. 2018;24:6195-203.
24. Liao Y, Tsai C, Huang H. Optimizing osimertinib for NSCLC: targeting resistance and exploring combination therapeutics. Cancers. 2025;17:459.
25. Cerbone L, Benitez JC, Planchard D, Genova C. An overview of osimertinib as a treatment of non-small cell lung cancer (NSCLC): an update. Expert Opin Pharmacother. 2021;22:809-19.
26. Veccia A, Dipasquale M, Lorenzi M, et al. Osimertinib in the treatment of epidermal growth factor receptor-mutant early and locally advanced stages of non-small-cell lung cancer: current evidence and future perspectives. Cancers. 2025;17:668.
27. Carlisle JW, Ramalingam SS. Role of osimertinib in the treatment of EGFR-mutation positive non-small-cell lung cancer. Future Oncol. 2019;15:805-16.
28. Nie N, Li J, Zhang J, et al. First-line osimertinib in patients with EGFR-mutated non-small cell lung cancer: effectiveness, resistance mechanisms, and prognosis of different subsequent treatments. Clin Med Insights Oncol. 2022;16:11795549221134735.
29. Pan K, Ramalingam SS. Rapidly evolving therapeutic advances for classical EGFR-mutant NSCLC. Front Oncol. 2025;15:1732467.
30. Li L, Huang Q, Sun J, et al. Efficacy and safety of osimertinib for patients with EGFR-mutated NSCLC: a systematic review and meta-analysis of randomized controlled studies. Acta Oncol. 2022;61:1347-53.
31. Yi L, Fan J, Qian R, Luo P, Zhang J. Efficacy and safety of osimertinib in treating EGFR‐mutated advanced NSCLC: a meta‐analysis. Int J Cancer. 2019;145:284-94.
32. Liu J, Li X, Shao Y, Guo X, He J. The efficacy and safety of osimertinib in treating nonsmall cell lung cancer: A PRISMA-compliant systematic review and meta-analysis. Medicine. 2020;99:e21826.
33. Chen P, Chen F, Lei J, Zhou B. Curative effectiveness and safety of osimertinib in the treatment for non-small cell lung cancer: a meta-analysis of the experimental evidence. Onco Targets Ther. 2018;11:9033-47.
34. Huang L, Huang H, Zhou X, et al. Osimertinib or EGFR-TKIs/chemotherapy in patients with EGFR-mutated advanced nonsmall cell lung cancer: a meta-analysis. Medicine. 2019;98:e17705.
35. Wang N, Zhang Y, Mi Y, et al. Osimertinib for EGFR-mutant lung cancer with central nervous system metastases: a meta-analysis and systematic review. Ann Palliat Med. 2020;9:3038-47.
36. Zhang H, Chen J, Liu T, Dang J, Li G. First-line treatments in EGFR-mutated advanced non-small cell lung cancer: a network meta-analysis. PLoS ONE. 2019;14:e0223530.
37. Holleman MS, Van Tinteren H, Groen HJM, Al MJ, Uyl-de Groot CA. First-line tyrosine kinase inhibitors in EGFR mutation-positive non-small-cell lung cancer: a network meta-analysis. Onco Targets Ther 2019;12:1413-21.
38. Qureshi Z, Altaf F, Jamil A, Siddique R. Meta-analysis of targeted therapies in EGFR-mutated non-small cell lung cancer: efficacy and safety of osimertinib, erlotinib, and gefitinib as first-line treatment. Am J Clin Oncol. 2025;48:44-54.
39. Zhao M, Zhang J, Gao J, Wang J, Ma Z. Osimertinib efficacy and safety in treating epidermal growth factor receptor mutation-positive advanced non-small‐cell lung cancer: a meta-analysis. Clin Pharm Drug Dev. 2024;14:5-10.
40. Priantti JN, Fujiwara Y, Aquino De Moraes FC, et al. Safety and efficacy of osimertinib in patients with non-small-cell lung cancer and uncommon tumoral epidermal growth factor receptor mutations: a systematic review and single-arm meta-analysis. JCO Precis Oncol. 2024;8:e2400331.
41. Cui S, Zhang Y, Liu L, et al. The efficacy and safety of Osimertinib in advanced non-small cell lung cancer patients with Thr790Met resistance mutations: a systematic review and meta-analysis. Ann Palliat Med. 2021;10:1851-60.
42. Tan DS, Nadal E, Cheema P, et al. TROPION-lung15: a randomized phase III study of osimertinib combined with datopotamab deruxtecan (Dato-DXd) or Dato-DXd alone versus platinum-doublet chemotherapy in patients withEGFR-mutated advanced non-small cell lung cancer and whose disease has progressed on prior osimertinib. Ther Adv Med Oncol. 2025;17:17588359251385410.
43. Ríos-Hoyo A, Moliner L, Arriola E. Acquired mechanisms of resistance to osimertinib -the next challenge. Cancers. 2022;14:1931.
44. Tsubata Y, Tanino R, Isobe T. Current therapeutic strategies and prospects for EGFR mutation-positive lung cancer based on the mechanisms underlying drug resistance. Cells. 2021;10:3192.
45. He J, Huang Z, Han L, Gong Y, Xie C. Mechanisms and management of 3rd‑generation EGFR‑TKI resistance in advanced non‑small cell lung cancer (Review). Int J Oncol. 2021;59:90.
46. Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27:146-55.
47. Wu Y, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383:1711-23.
48. Herbst RS, Wu Y, John T, et al. Adjuvant osimertinib for resected EGFR-mutated stage IB-IIIA non-small-cell lung cancer: updated results from the phase III randomized ADAURA trial. J Clin Oncol. 2023;41:1830-40.
49. Herbst RS, Tsuboi M, John T, et al. Overall survival analysis from the ADAURA trial of adjuvant osimertinib in patients with resected EGFR-mutated (EGFRm) stage IB-IIIA non-small cell lung cancer (NSCLC). J Clin Oncol. 2023;41:LBA3.
50. Tsuboi M, Herbst RS, John T, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med. 2023;389:137-47.
51. Xie J, Chen C, Zhang B, et al. Abstract CT164: efficacy and safety of osimertinib therapy in high-risk stage I EGFRm NSCLC after R0 resection (OSTAR): a phase II, prospective, single-arm study. Cancer Res. 2025;85:CT164.
52. Blakely CM, Urisman A, Gubens MA, et al. Neoadjuvant osimertinib for the treatment of stage I-IIIA epidermal growth factor receptor-mutated non-small cell lung cancer: a phase II multicenter study. J Clin Oncol. 2024;42:3105-14.
53. Aredo JV, Urisman A, Gubens MA, et al. Phase II trial of neoadjuvant osimertinib for surgically resectable EGFR-mutated non-small cell lung cancer. J Clin Oncol. 2023;41:8508.
54. Lyu C, Fang W, Ma H, et al. Osimertinib as neoadjuvant treatment for resectable stage II-IIIB EGFR mutant lung adenocarcinoma (NEOS). J Clin Oncol. 2021;39:8524.
55. Lu S, Kato T, Dong X, et al. Osimertinib after chemoradiotherapy in stage III EGFR-mutated NSCLC. N Engl J Med. 2024;391:585-97.
56. Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382:41-50.
57. Planchard D, Boyer MJ, Lee J, et al. Postprogression outcomes for osimertinib versus standard-of-care EGFR-TKI in patients with previously untreated EGFR-mutated advanced non-small cell lung cancer. Clin Cancer Res. 2019;25:2058-63.
58. Reungwetwattana T, Nakagawa K, Cho BC, et al. CNS response to osimertinib versus standard epidermal growth factor receptor tyrosine kinase inhibitors in patients with untreated EGFR-mutated advanced non-small-cell lung cancer. J Clin Oncol. 2018;36:3290-7.
59. Planchard D, Jänne PA, Cheng Y, et al. Osimertinib with or without chemotherapy in EGFR-mutated advanced NSCLC. N Engl J Med. 2023;389:1935-48.
60. Jänne PA, Planchard D, Kobayashi K, et al. Survival with osimertinib plus chemotherapy in EGFR-mutated advanced NSCLC. N Engl J Med. 2026;394:27-38.
61. Saito R, Sugawara S, Ko R, et al. Phase 2 study of osimertinib in combination with platinum and pemetrexed in patients with previously untreated EGFR-mutated advanced non-squamous non-small cell lung cancer: the OPAL Study. Eur J Cancer. 2023;185:83-93.
62. Fukui T, Mamesaya N, Takahashi T, et al. A prospective phase II trial of first-line osimertinib for patients with EGFR mutation-positive NSCLC and poor performance status (OPEN/TORG2040). J Thorac Oncol. 2025;20:665-75.
63. Mamesaya N, Fukui T, Takahashi T, et al. A multicenter, prospective phase II trial of first-line osimertinib treatment for patients with poor performance status and EGFR mutation-positive non-small cell lung cancer (OPEN/TORG2040). J Clin Oncol. 2024;42:8552.
64. Park C, Cho H, Choi Y, Oh I, Kim Y. A phase II trial of osimertinib as the first-line treatment of non-small cell lung cancer harboring activating EGFR mutations in circulating tumor DNA: liquidlung-O-cohort 1. Cancer Res Treat. 2021;53:93-103.
65. Mok TS, Wu Y, Ahn M, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. 2017;376:629-40.
66. Akamatsu H, Katakami N, Okamoto I, et al. Osimertinib in Japanese patients with EGFR T790M mutation‐positive advanced non‐small‐cell lung cancer: AURA3 trial. Cancer Sci. 2018;109:1930-8.
67. Yang JC, Ahn M, Kim D, et al. Osimertinib in pretreated T790M-positive advanced non-small-cell lung cancer: AURA study phase II extension component. J Clin Oncol. 2017;35:1288-96.
68. Park C, Cho H, Choi Y, Oh I, Kim Y. A phase II trial of osimertinib in the second-line treatment of non-small cell lung cancer with the EGFR T790M mutation, detected from circulating tumor DNA: LiquidLung-O-cohort 2. Cancer Res Treat. 2019;51:777-87.
69. Ahn M, Han J, Kim D, et al. Osimertinib in patients with T790M-positive advanced non-small cell lung cancer: Korean subgroup analysis from phase II studies. Cancer Res Treat. 2020;52:284-91.
70. Cho JH, Lim SH, An HJ, et al. Osimertinib for Patients with non-small-cell lung cancer harboring uncommon EGFR mutations: a multicenter, open-label, phase II trial (KCSG-LU15-09). J Clin Oncol. 2020;38:488-95.
71. Okuma Y, Kubota K, Shimokawa M, et al. First-line osimertinib for previously untreated patients with NSCLC and uncommon EGFR mutations: the UNICORN phase 2 nonrandomized clinical trial. JAMA Oncol. 2024;10:43.
72. Okuma Y, Kubota K, Shimokawa M, et al. Uncommon EGFR mutations conducted with osimertinib in patients with NSCLC (UNICORN): a phase 2 study. J Clin Oncol. 2023;41:9045.
73. Eide IJZ, Stensgaard S, Helland Å, et al. Osimertinib in non-small cell lung cancer with uncommon EGFR-mutations: a post-hoc subgroup analysis with pooled data from two phase II clinical trials. Transl Lung Cancer Res. 2022;11:953-63.
74. Kim TM, Ock CY, Kim M, et al. 1529P - phase II study of osimertinib in NSCLC patients with EGFR exon 20 insertion mutation: A multicenter trial of the Korean cancer study group (LU17-19). Ann Oncol. 2019;30:v628.
75. Bhatt VR, D’souza SP, Smith LM, et al. Epidermal growth factor receptor mutational status and brain metastases in non-small-cell lung cancer. J Glob Oncol. 2017;3:208-17.
76. Wu Y, Ahn M, Garassino MC, et al. CNS efficacy of osimertinib in patients with T790M-positive advanced non-small-cell lung cancer: data from a randomized phase III trial (AURA3). J Clin Oncol. 2018;36:2702-9.
77. Xing L, Pan Y, Shi Y, et al. Biomarkers of osimertinib response in patients with refractory, EGFR-T790M-positive non-small cell lung cancer and central nervous system metastases: the APOLLO study. Clin Cancer Res. 2020;26:6168-75.
78. Marinis FD, Wu Y, De Castro G, et al. ASTRIS: a global real-world study of osimertinib in >3000 patients with EGFR T790M positive non-small-cell lung cancer. Future Oncol. 2019;15:3003-14.
79. Lee JH, Kim EY, Park C, et al. Real-world study of osimertinib in Korean patients with epidermal growth factor receptor T790M mutation-positive non-small cell lung cancer. Cancer Res Treat. 2023;55:112-22.
80. Zhang D, Liu X, Shen F, et al. Osimertinib versus comparator first-generation epidermal growth factor receptor tyrosine kinase inhibitors as first-line treatment in patients with advanced EGFR-mutated non-small cell lung cancer: a Chinese, multicenter, real-world cohort study. Transl Lung Cancer Res. 2023;12:2229-44.
81. Chang G, Shih J, Yu C, et al. Real-world osimertinib pretreatment experience in patients with epidermal growth factor receptor T790M mutation-positive locally advanced or metastatic non-small cell lung cancer. PLoS ONE. 2024;19:e0303046.
82. Chen H, Chen C, Liao W, et al. Optimal first-line treatment for EGFR-mutated NSCLC: a comparative analysis of osimertinib and second-generation EGFR-TKIs. BMC Pulm Med. 2024;24:517.
83. Tiwari A, Singh AK, Noronha V, et al. Real-world experience of first-line osimertinib in EGFR mutated non-small cell lung cancers from a tertiary cancer center, India. South Asian J Cancer. 2024;14:785-90.
84. Yu HA, Arcila ME, Rekhtman N, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19:2240-7.
85. Takahama T, Azuma K, Shimokawa M, et al. Plasma screening for the T790M mutation ofEGFR and phase 2 study of osimertinib efficacy in plasma T790M-positive non-small cell lung cancer: west Japan Oncology Group 8815L/LPS study. Cancer. 2020;126:1940-8.
86. Tsuboi M, Weder W, Escriu C, et al. Neoadjuvant osimertinib with/without chemotherapy versus chemotherapy alone for EGFR-mutated resectable non-small-cell lung cancer: NeoADAURA. Future Oncol. 2021;17:4045-55.
87. Nicoś M, Sroka-bartnicka A, Kalinka E, Krawczyk P. Possibilities of overcoming resistance to osimertinib in NSCLC patients with mutations in the EGFR gene. Cancers. 2025;17:563.
88. Yamaguchi T, Masago K, Sasaki E, Kuroda H, Matsushita H, Horio Y. EML4-ALK variant 3a/b as a mechanism of osimertinib resistance in a patient with EGFR L858R positive NSCLC. Cancer Genet. 2024;280-1:13-6.
89. Ntzifa A, Marras T, Georgoulias V, Lianidou E. Liquid biopsy for the management of NSCLC patients under osimertinib treatment. Crit Rev Clin Lab Sci. 2024;61:347-69.
90. Zhang W, Xiong J, Li Y, et al. Efficacy and safety of distinct regimens for individuals with advanced EGFR-mutated non-small-cell lung cancer who progressed on EGFR tyrosine-kinase inhibitors: a systematic review and network meta-analysis. Ther Adv Med Oncol. 2025;17:17588359251338046.
91. Passaro A, Wang J, Wang Y, et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann Oncol. 2024;35:77-90.
92. Yu HA, Goto Y, Hayashi H, et al. HERTHENA-Lung01, a phase II trial of patritumab deruxtecan (HER3-DXd) in epidermal growth factor receptor-mutated non-small-cell lung cancer after epidermal growth factor receptor tyrosine kinase inhibitor therapy and platinum-based chemotherapy. J Clin Oncol. 2023;41:5363-75.
93. Sands J, Ahn M, Lisberg A, et al. Datopotamab deruxtecan in advanced or metastatic non-small cell lung cancer with actionable genomic alterations: results from the phase II TROPION-Lung05 study. J Clin Oncol. 2025;43:1254-65.
94. Hartmaier RJ, Markovets AA, Ahn MJ, et al. Osimertinib + savolitinib to overcome acquired MET-mediated resistance in epidermal growth factor receptor-mutated, MET-amplified non-small cell lung cancer: TATTON. Cancer Discov. 2023;13:98-113.
95. Yang JCH, Ellers-Lenz B, Straub J, Johne A, Wu YL. 536TiP - INSIGHT 2: tepotinib plus osimertinib in patients with EGFR-mutant NSCLC having acquired resistance to EGFR TKIs due to MET-amplification: a phase II trial in progress study. Ann Oncol. 2019;30:ix181.
96. Pan J, Cai X, Cao Z, Pan J, Zheng H. Osimertinib in the treatment of EGFR mutation-positive advanced non-small cell lung cancer: a meta-analysis. Pharmacology. 2023;108:8-16.
97. Lin J, Zhang C, Weng J, Wang S. Efficacy and safety of Osimertinib and other third-generation EGFR TKIs in advanced NSCLC: a systematic review and meta-analysis. Discov Oncol. 2026;17:232.
98. Zhao Y, Liu J, Cai X, et al. Efficacy and safety of first line treatments for patients with advanced epidermal growth factor receptor mutated, non-small cell lung cancer: systematic review and network meta-analysis. BMJ. 2019;367:l5460.
99. Alanazi A, Yunusa I, Elenizi K, Alzarea AI. Efficacy and safety of tyrosine kinase inhibitors in advanced non-small-cell lung cancer harboring epidermal growth factor receptor mutation: a network meta-analysis. Lung Cancer Manag. 2020;10:LMT43.
100. Xie T, Zou Z, Liu C, et al. Front-line therapy in EGFR exon 19 deletion and 21 Leu858Arg mutations in advanced non-small cell lung cancer: a network meta-analysis. Evid Based Complement Alternat Med. 2021;2021:1-15.
101. Chan S, Choi HC, Lee VH. Overall survival benefits of first-line treatments for Asian patients with advanced EGFR-mutated NSCLC harboring L858R mutation: a systematic review and network meta-analysis. JTO Clin Res Rep. 2022;3:100322.
102. Du W, Li A, Xiao B, et al. First‐line third‐generation EGFR tyrosine kinase inhibitor monotherapy for advanced EGFR‐mutated non‐small cell lung cancer: a systematic review and network meta‐analysis. MedComm. 2025;6:e70393.
103. Zhang W, Zhang X, Zhao W, et al. What is the optimal first-line regimen for advanced non-small cell lung cancer patients with epidermal growth factor receptor mutation: a systematic review and network meta-analysis. BMC Pulm Med. 2024;24:620.
104. Erickson A, Brastianos P, Das S. 04. Assessment of efficacy and safety of osimertinib for patients with intracranial metastatic disease: a systematic review and meta-analysis. Neuro Oncol Adv. 2020;2:ii1.
105. Liu L, Bai H, Seery S, et al. Efficacy and safety of treatment modalities across EGFR selected/unselected populations with non-small cell lung cancer and brain metastases: a systematic review and Bayesian network meta-analysis. Lung Cancer. 2021;158:74-84.
106. Ma J, Pang X, Zhang S, Huang L, Sun L, Han C. First-line treatment of EGFR-mutated non-small cell lung cancer with brain metastases: a systematic review and meta-analysis. Sci Rep. 2024;14:22901.
107. Mei T, Wang T, Xu T, Zhou Q. Comparing the effectiveness and safety of first-line interventions in patients with advanced epidermal growth factor receptor-mutant non-small cell lung cancer, with particular focus on brain metastatic status: a systematic review and network meta-analysis. Clin Oncol. 2025;40:103776.
108. Wen L, Zhen J, Shan C, et al. Efficacy and safety of osimertinib for leptomeningeal metastases from EGFR-mutant non-small cell lung cancer: a pooled analysis. Eur J Med Res. 2023;28:267.
109. Bian DJ, Lazaratos A, Maritan SM, et al. Osimertinib is associated with improved outcomes in pre-treated non-small cell lung cancer leptomeningeal metastases: a systematic review and meta-analysis. Heliyon. 2024;10:e29668.
110. Yi X, Song J, Gao R, et al. Efficacy of osimertinib in EGFR-mutated advanced non-small-cell lung cancer with different T790M status following resistance to prior EGFR-TKIs: a systematic review and meta-analysis. Front Oncol. 2022;12:863666.
111. Priantti JN, Vilbert M, Moraes FCA, et al. Safety and efficacy of osimertinib in patients with NSCLC and uncommon tumoral EGFR mutations: a systematic review and meta-analysis. J Clin Oncol. 2024;42:8642.
112. Song C, Yang X. Osimertinib-centered therapy against uncommon epidermal growth factor receptor-mutated non-small-cell lung cancer- a mini review. Front Oncol. 2022;12:834585.
113. Zhou G, Guo L, Xu J, Tang K, Chen J. Comparison of osimertinib plus bevacizumab against osimertinib alone in NSCLC harboring EGFR mutations: a systematic review and meta-analysis. Ther Adv Med Oncol. 2024;16:17588359241227677.
114. Yao L, Zhang C, Li D, Xu L, Yang X. Efficacy and safety of osimertinib plus bevacizumab versus osimertinib alone for advanced non-small-cell lung cancer with EGFR mutations: a meta-analysis of randomized controlled trials. Medicine. 2024;103:e40320.
115. Qi Y, Xia X, Shao L, et al. An updated network meta-analysis of EGFR-TKIs and combination therapy in the first-line treatment of advanced EGFR mutation positive non-small cell lung cancer. Front Oncol. 2022;12:616546.
116. Grazini U, Markovets A, Ireland L, et al. Overcoming osimertinib resistance with akt inhibition in EGFRm-driven non-small cell lung cancer with PIK3CA/PTEN alterations. Clin Cancer Res. 2024;30:4143-54.
117. Peled N, Tufman A, Sequist L, et al. COMPEL: osimertinib plus platinum-based chemotherapy in patients with EGFR-mutated advanced NSCLC and progression on first-line osimertinib. ESMO Open. 2025;10:105807.
118. Deng S, Sun C, Liu D, et al. Antibody-drug conjugates: a new twist to overcome EGFR-TKIs resistance in non-small cell lung cancer. Pharmacol Res. 2026;223:108066.
119. Wang R, Chen Y, Li L, Zhang L, Zhang S. Osimertinib acquired resistance among patients with EGFR-mutated NSCLC: from molecular mechanisms to clinical therapeutic strategies. Cancer Drug Resist. 2025;8:61.
120. Maione P, Romano FJ, Gridelli C. Amivantamab plus lazertinib and platin-based chemotherapy plus osimertinib in EGFR-mutant NSCLC: how to choose among them and when is monotherapy with osimertinib still the best option? Curr Oncol. 2026;33:54.
121. Sankar K, Waissengrin B, Reckamp KL. The expanding landscape of next-generation EGFR tyrosine kinase inhibitors: have we reached capacity? J Thorac Oncol. 2025;20:1569-72.
122. Wang C, Wu W, Yan B, et al. The causal relationship between epigenetic aging and osteoporosis: a bi-directional Mendelian randomization study. J Transl Genet Genom. 2025;9:90-9.
123. Karri V, Dalia SM. Persistent IFN-γ signaling in acquired resistance to PD-(L)1 blockade in NSCLC. J Transl Genet Genom. 2025;9:352-8.
124. Prakashan D, PR R, Kaushik A, Gandhi S. Sustainable nanotechnology and artificial intelligence to empower image-guided therapy for precision healthcare. BME Front. 2025;6:0150.
125. Zhu H, Wang R, Qian J, et al. Leveraging large language models for predicting postoperative acute kidney injury in elderly patients. BME Front. 2025;6:0111.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.